35 - Adapting a Brief Adolescent Relationship Abuse Intervention for the Emergency Department: Youth, Parent, and Staff Perspectives
Friday, April 22, 2022
6:15 PM – 8:45 PM US MT
Poster Number: 35 Publication Number: 35.103
Kimberly A. Randell, Children's Mercy Hospitals and Clinics, Kansas City, MO, United States; Melissa Miller, Children's Mercy Hospitals and Clinics, Kansas City, MO, United States; Lauren Arney, Children's Mercy Hospitals and Clinics, Kansas City, MO, United States; Megan E. Cunningham, CMH, Westwood, KS, United States; Ashlyn Lipnicky, University of Kansas School of Medicine, Kansas City, KS, United States; Elizabeth Miller, UPMC Childrens Hospital of Pittsburgh, Pittsburgh, PA, United States; Ann M. Davis, Center for Children's Healthy Lifestyles & Nutrition/ KU Medical Center, Kansas City, MO, United States; Megha Ramaswamy, University of Kansas School of Medicine, Kansas City, KS, United States
Objective: To explore youth, parent, and ED staff perspectives on adaptation for ED use of Healthcare Education Assessment and Response for Teen Relationships (HEART), an evidence-based, brief, universal education ARA intervention originally designed for school health centers.
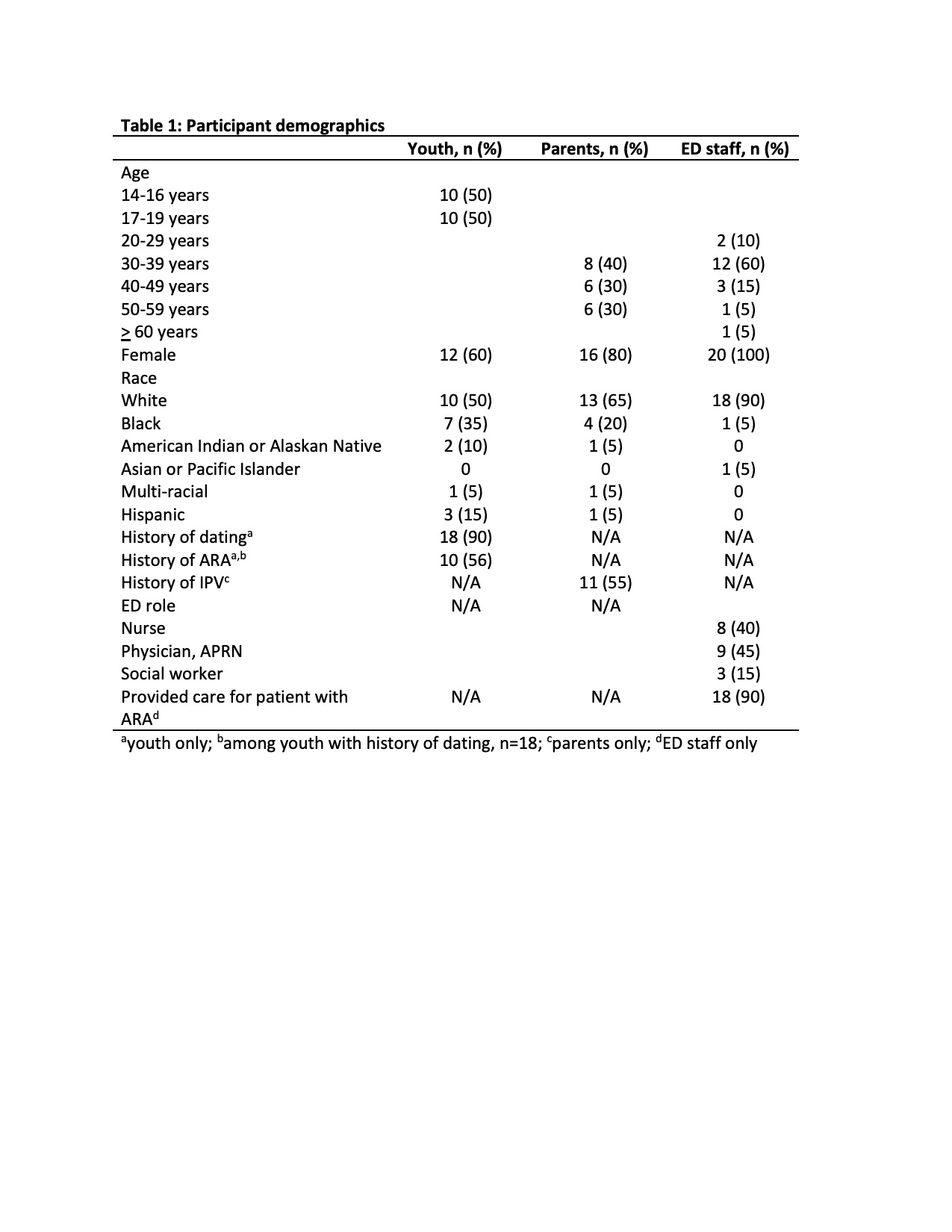
Design/Methods: We conducted individual interviews with youth aged 14-19 years seeking ED care, parents of such youth, and ED staff (n=20 each). We recruited and interviewed youth and parents during an ED visit. ED staff were recruited via email and meeting announcements and interviewed via video platform. Interviews included a demonstration of HEART. We used a thematic analysis approach to code interview transcripts and then consolidate codes into themes.
Results: Participants (Table 1) in all groups felt that ARA is an important issue that children’s hospitals should address. All groups found ED implementation of HEART acceptable, noting it provided important information and could facilitate ARA resource access. Participants described individual-level (e.g., discomfort discussing ARA and/or adolescent sexuality, lack of staff buy-in) and system-level (e.g., time constraints, staff workload) barriers to HEART in the ED. Potential implementation facilitators included staff champions and aligning delivery with current ED practices. Participants in all groups supported confidential HEART delivery as designed, although parents and ED staff noted that parents also typically want to know about their adolescents’ romantic relationships. Reflecting HEART implementation guidelines, youth shared benefits of parent support after ARA disclosure but recommended shared decision making with the youth about potential benefit of this. Participants in all groups recommended modifying HEART by excluding some patients from universal delivery (e.g., severe illness, evaluation for acute sexual assault). Acceptability of discussing ED point-of-care harm reduction resources (e.g., emergency contraception, condoms) as part of HEART varied, with some youth, parents, and ED staff expressing ambivalence or disapproval of these. See Table 2 for illustrative quotes.Conclusion(s): Youth, parents, and ED staff found ED implementation of HEART acceptable, identified implementation barriers and facilitators, and offered guidance on tailoring HEART to fit the ED setting. Findings affirm the value of engaging youth, parents, and healthcare teams in the early stages of intervention adaptation. Table 1: Participant demographics Table 2: Illustrative Quotes

 photo")
.jpg)