
Neonatal Quality Improvement
Category: Abstract Submission
Neonatal Quality Improvement I

Aditi Dey, MD
Neonatal Perinatal Medicine Fellow
Johns Hopkins All Childrens' Hospital
Saint Petersburg, Florida, United States
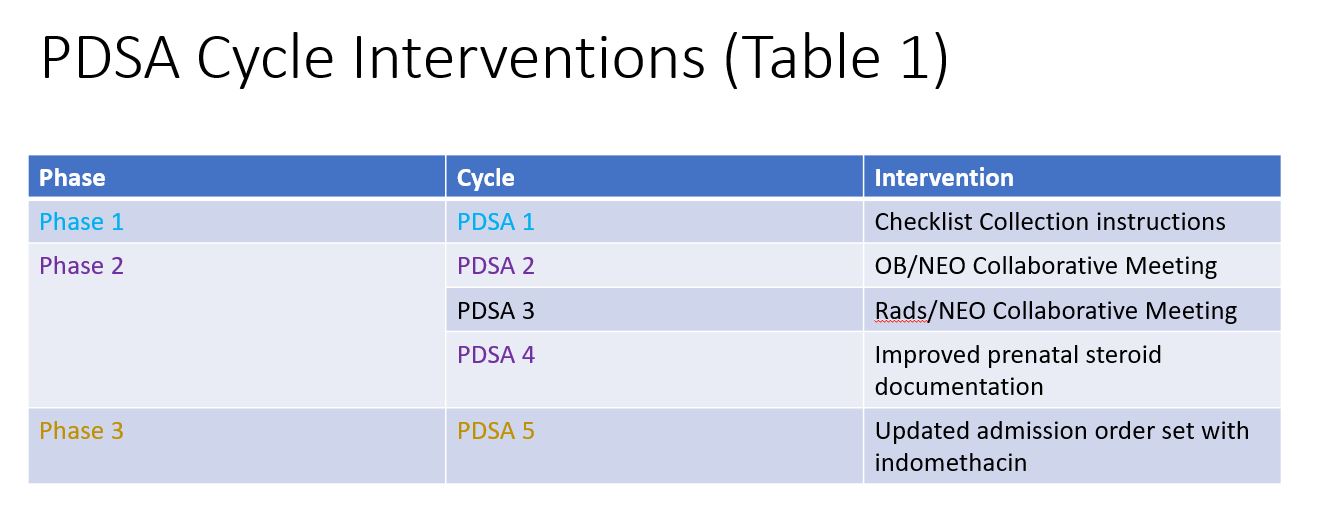 Description of the three phase initiative and corresponding PDSA cycles for each phase
Description of the three phase initiative and corresponding PDSA cycles for each phase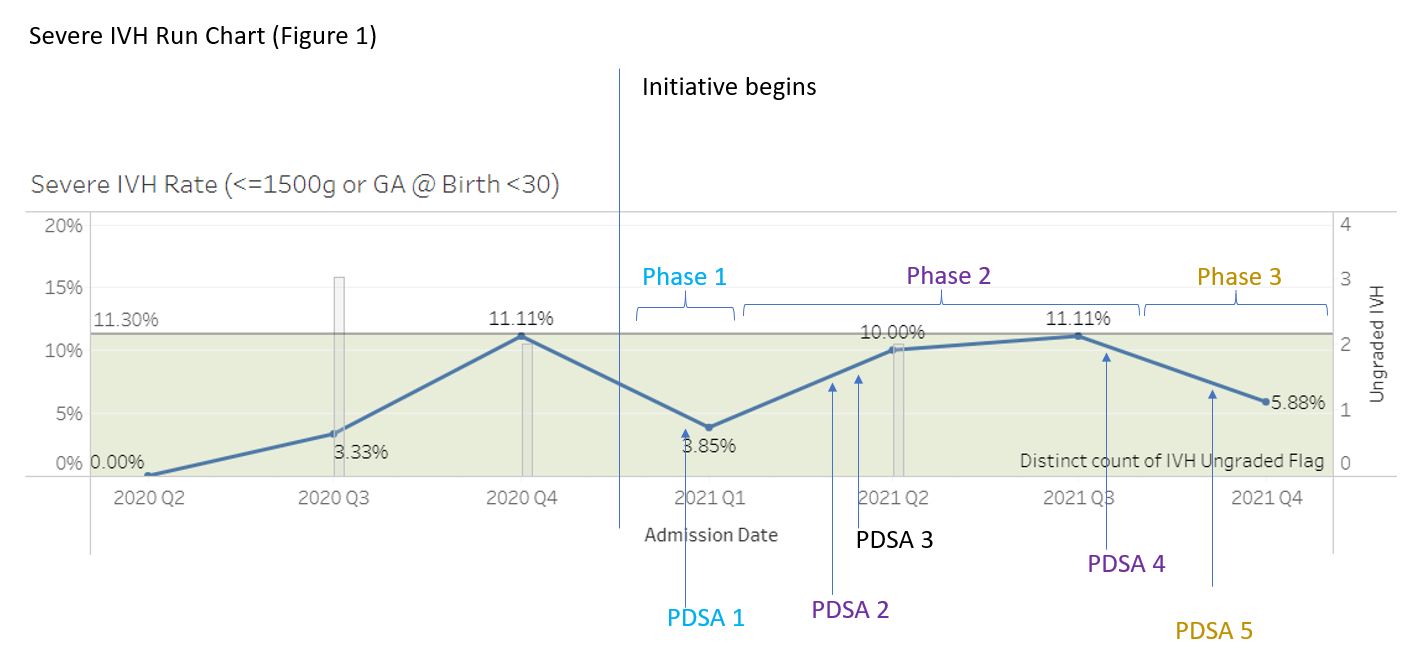 Run chart of rate of severe IVH. Average rate of IVH for the two years prior to the initiative was 11.3%. The grey bar graph demonstrates cranial ultrasounds that had unclear radiological interpretations. Following the QI initiative, there was reduction in severe IVH and number of unclear readings of cranial ultrasounds.
Run chart of rate of severe IVH. Average rate of IVH for the two years prior to the initiative was 11.3%. The grey bar graph demonstrates cranial ultrasounds that had unclear radiological interpretations. Following the QI initiative, there was reduction in severe IVH and number of unclear readings of cranial ultrasounds.