
Global Neonatal & Children's Health
Category: Abstract Submission
Global Child and Adolescent Health I

Osayame A. Ekhaguere, M.D., MPH
Neonatologist
Riley Hospital for Children at Indiana Univeristy Health
Carmel, IN, United States
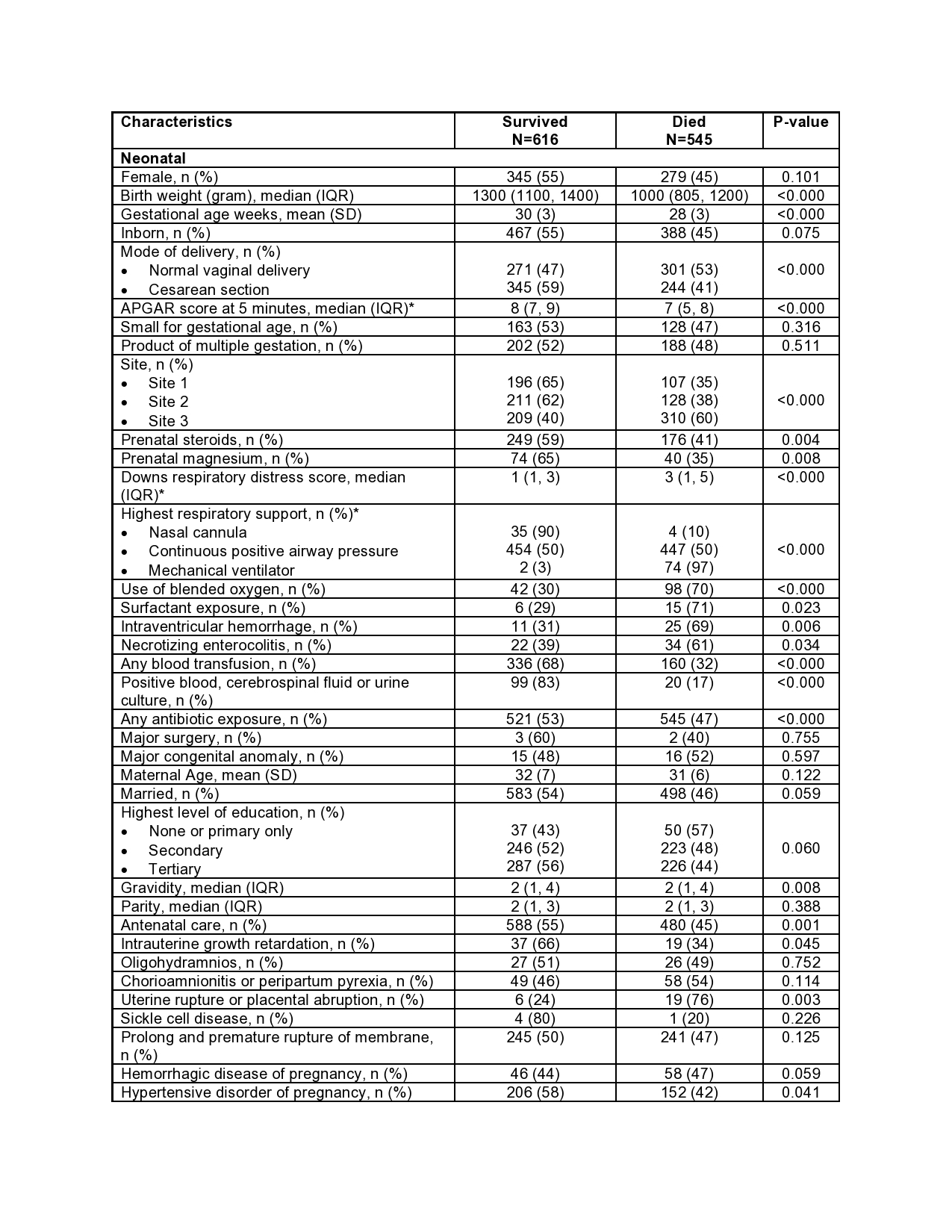 *Variables with ≥10% missing values
*Variables with ≥10% missing values.jpg) *Mechanical ventilator exposure was not included in the model due to a lack of convergence. Almost all subjects placed on the ventilator died
*Mechanical ventilator exposure was not included in the model due to a lack of convergence. Almost all subjects placed on the ventilator died