
Neonatal Infectious Diseases/Immunology
Category: Abstract Submission
Neonatal Infectious Diseases/Immunology: CMV, HIV, Syphilis, Immunology
 photo")
Timothy J. Boly, DO (he/him/his)
Instructor of Pediatrics
University of Iowa
Iowa City, IA, United States
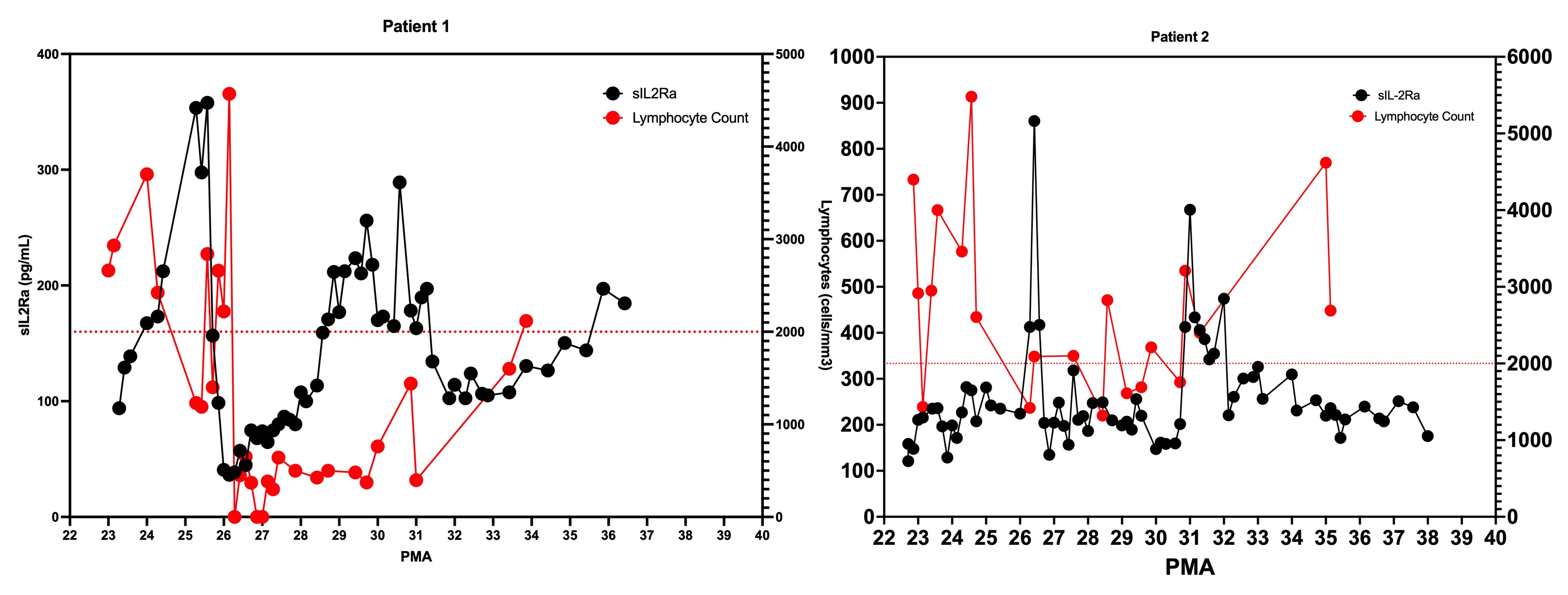 Serum sIL2Ra levels (left axis) as compared to peripheral lymphocyte count (right axis) for Patients 1 and 2. During periods of elevated sIL2Ra, there is an associated decrease in lymphocytes. Horizontal dashed line represents lymphopenia threshold.
Serum sIL2Ra levels (left axis) as compared to peripheral lymphocyte count (right axis) for Patients 1 and 2. During periods of elevated sIL2Ra, there is an associated decrease in lymphocytes. Horizontal dashed line represents lymphopenia threshold.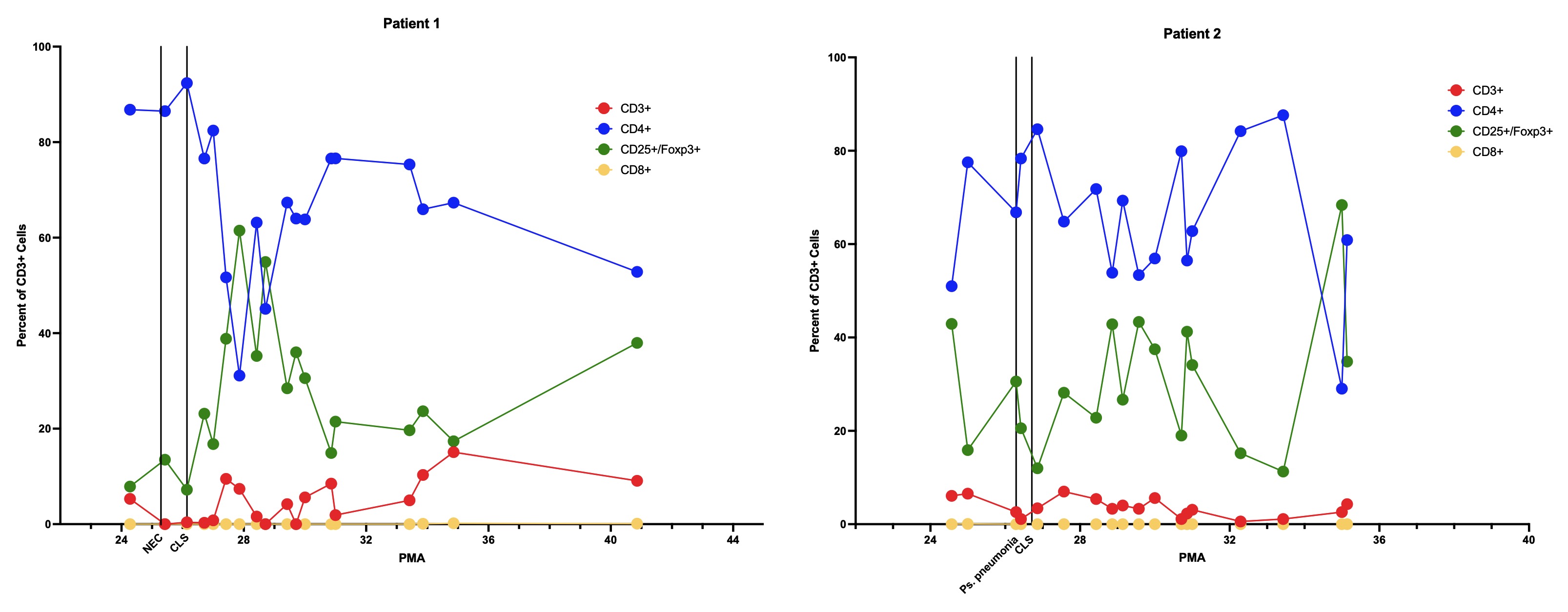 Subpopulations of T lymphocytes, expressed as percent of total CD3+ cells. Red: CD3+ only; blue: CD4+; green: CD25+/Foxp3+; yellow: CD8+. Significant illness and onset of CLS expressed by vertical lines.
Subpopulations of T lymphocytes, expressed as percent of total CD3+ cells. Red: CD3+ only; blue: CD4+; green: CD25+/Foxp3+; yellow: CD8+. Significant illness and onset of CLS expressed by vertical lines.