
Neonatal Quality Improvement
Category: Abstract Submission
Neonatal Quality Improvement II: Neurology and Infection

Johanan Vargas, MD MBA
Associate Professor
Johns Hopkins University School of Medicine
Riverview, Florida, United States
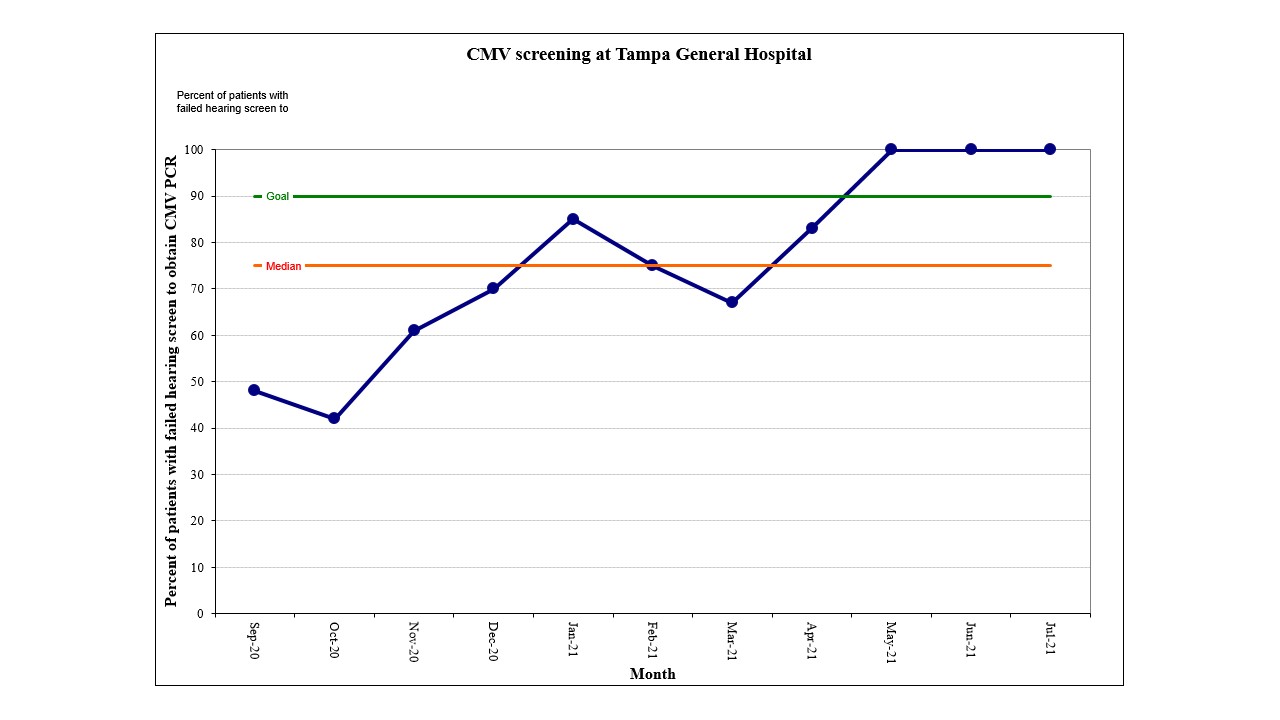 Percentage of infants who had a CMV PCR resulted after failing their hearing screen in one or both ears prior to discharge.
Percentage of infants who had a CMV PCR resulted after failing their hearing screen in one or both ears prior to discharge.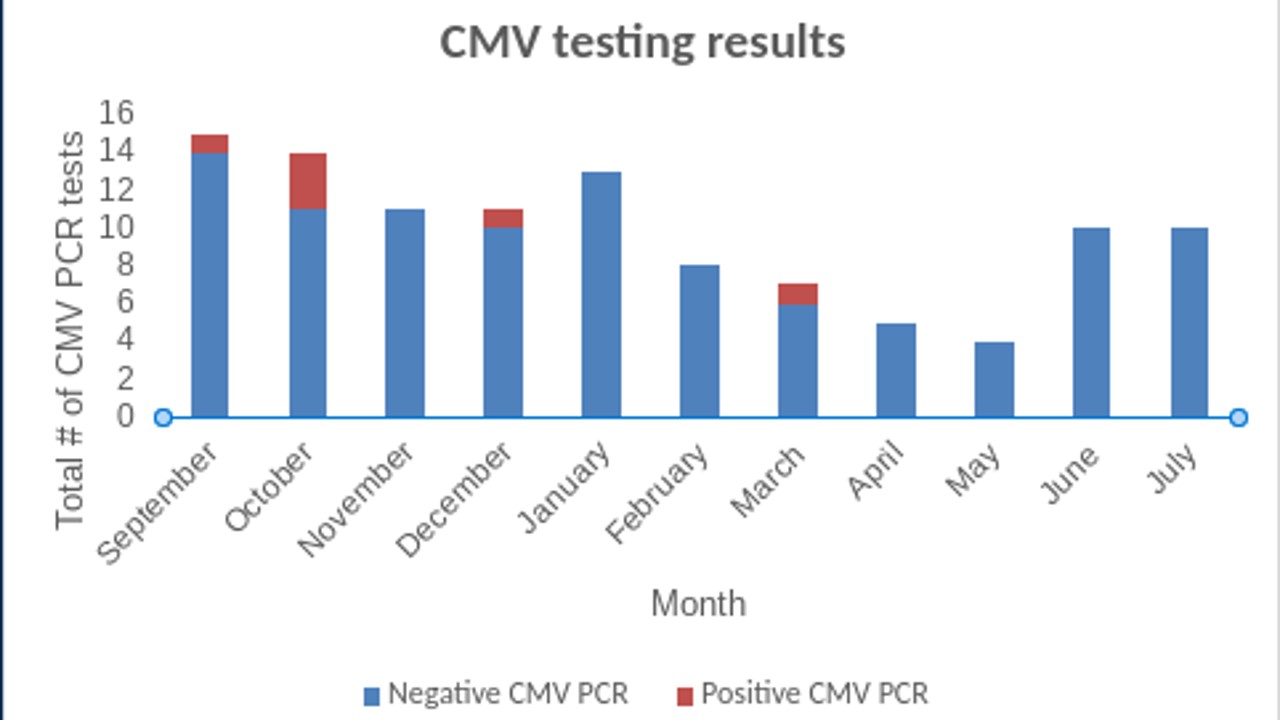 Number of positive CMV PCR results among those with failed hearing screens
Number of positive CMV PCR results among those with failed hearing screens