
Emergency Medicine: All Areas
Category: Abstract Submission
Emergency Medicine VI
YARON FINKELSTEIN, MD
The Hospital for Sick Children
TORONTO, Ontario, Canada
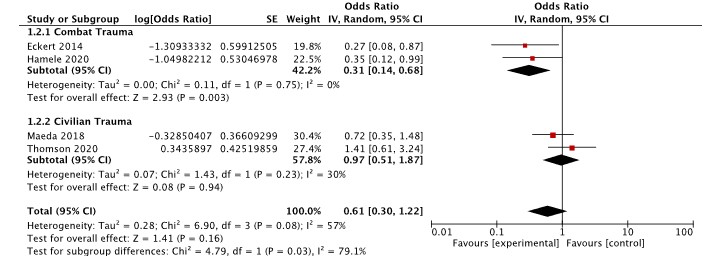 *Adjusted for mechanism, ISS, serum base deficit, hypotension, and GCS score
*Adjusted for mechanism, ISS, serum base deficit, hypotension, and GCS score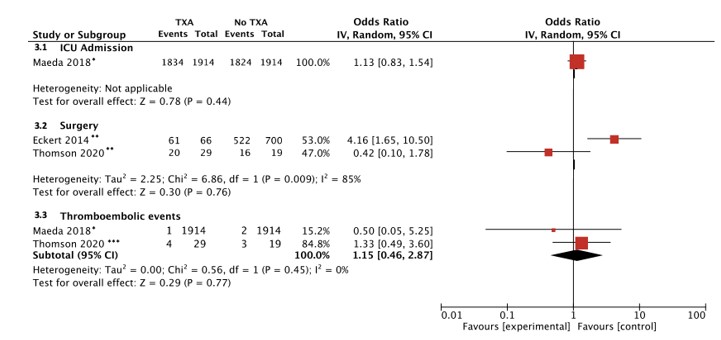 * Propensity matching based on age, gender, body weight, height, trauma sites, hospital type, PICU admission, ambulance transfer, and hospital volume
* Propensity matching based on age, gender, body weight, height, trauma sites, hospital type, PICU admission, ambulance transfer, and hospital volume