
Neonatal/Infant Resuscitation
Category: Abstract Submission
Neonatal/Infant Resuscitation III
 photo")
Georgina L. Blochlinger, BSci BBMed(Hons)
Research Assistant
Royal Women's Hospital
Mount Eliza, Victoria, Australia
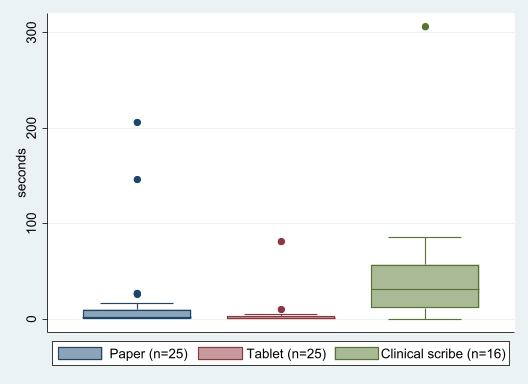 Graph shows box plots for each tool, centre horizontal line represents median, upper and lower edges of box show IQR, whiskers show the range, dots represent outliers. n=25 infants had a face mask applied, however not all of these were documented by each tool. p values shown on graph.
Graph shows box plots for each tool, centre horizontal line represents median, upper and lower edges of box show IQR, whiskers show the range, dots represent outliers. n=25 infants had a face mask applied, however not all of these were documented by each tool. p values shown on graph.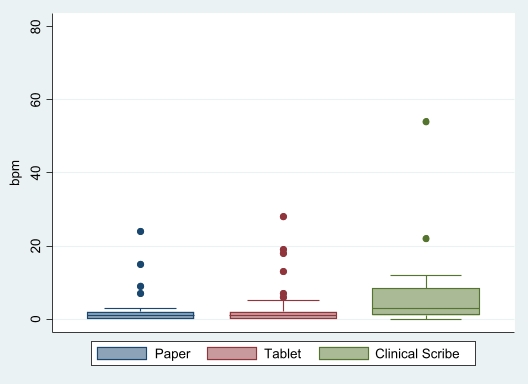 Graph shows box plots for each tool, centre horizontal line represents median, upper and lower edges of box show IQR, whiskers show the range, dots represent outliers. p values shown on graph.
Graph shows box plots for each tool, centre horizontal line represents median, upper and lower edges of box show IQR, whiskers show the range, dots represent outliers. p values shown on graph.