8 - Impact of Trainee Involvement On Safety Outcomes Of ERCP Procedures: A Multicenter Analysis From The Pediatric ERCP Initiative
Saturday, April 23, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 8 Publication Number: 8.207
Rekha K. Gupta, Johns Hopkins All Children's Hospital, St Petersburg, FL, United States; Racha T. Khalaf, University of South Florida, Tampa, FL, United States; John M. Morrison, Johns Hopkins All Children's Hospital, Saint Petersburg, FL, United States; Wenly Ruan, Baylor College of Medicine, Houston, TX, United States; Douglas S. Fishman, Baylor College of Medicine, Houston, TX, United States; Quin Liu, Cedars-Sinai Medical Center, Los Angeles, CA, United States; Bradley Barth, University of Texas Southwestern Medical School, Dallas, TX, United States; Matthew J. Giefer, The University of Queensland / Louisiana State University, New Orleans, LA, United States; Kyung Mo Kim, Asan Med Ctr, Seoul, Seoul-t'ukpyolsi, Republic of Korea; Mercedes Martinez, Columbia University, New York, NY, United States; Samuel Bitton, Cohen Children's Medical Center, lake success, NY, United States; Kulwinder Dua, Medical College of Wisconsin, Milwaukee, WI, United States; Clifton Huang, Cook Children's Medical Center/ Texas Christian University, Fort Worth, TX, United States; Petar Mamula, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Yuhua Zheng, Children's Hospital & Medical Center, los angeles, CA, United States; Travis L. Piester, Keck School of Medicine of the University of Southern California, Los Angeles, CA, United States; Amit S. Grover, Boston Children's Hospital, Harvard Medical School, Boston, MA, United States; Victor L. Fox, Harvard Medical School, Boston, MA, United States; Michael J. Wilsey, USF Health Morsani College of Medicine, St. Petersburg, FL, United States; David M. Troendle, UT Southwestern Medical Center/Children's Health, Dallas, TX, United States
Resident Johns Hopkins All Children's Hospital St Petersburg, Florida, United States
Background: The number of advanced endoscopy training programs for pediatric endoscopic retrograde cholangiopancreatography (ERCP) in the United States and Europe is increasing. Prior studies evaluating safety outcomes in pediatric ERCP have been limited by their retrospective nature, single center environment, and small numbers of overall procedures.
Objective: To determine if trainee involvement with ERCP affects 1) technical success of the procedure, 2) rates of post-procedural adverse outcomes, and 3) procedure duration
Design/Methods: Consecutive ERCPs on children < 19 years of age from 18 IRB-approved centers were entered prospectively into a REDCap database, as part of the Pediatric ERCP Database Initiative (PEDI). A secondary analysis was performed comparing technical success, post-procedural adverse event rates (defined by the American Society for Gastrointestinal Endoscopy (ASGE) lexicon), and procedure duration between cases with trainees to those without. Univariate and multivariable logistic and linear regression analysis was performed, where appropriate, accounting for any confounding effects of age at time of ERCP, trainee involvement, ASGE difficulty grade and presence of native papilla. A significance level of 0.05 was used.
Results: 28% (320/1124) of ERCP cases had trainee involvement. Demographic information summarized in Table 1 showed no significant difference in age, sex, or weight between cases with and without trainees (p >.05); however, the distribution of race did differ significantly between groups(p < .01). The presence of trainees did not impact technical success (OR =1.1 [95% CI 0.7, 1.8]; p=.65) or adverse events (OR= 1.2 [95% CI 0.8,1.9]; p=.43). Although fewer trainees were present in the top quartile ( >58 min.) of procedural time (19% vs. 26%; p=.02), procedure time did not remain different after controlling for confounding variables, including age at time of ERCP, ASGE difficulty grade and native papilla(p=0.06). Higher ASGE difficulty grade (3, 4, or 5 compared to 1 or 2) was associated with longer procedure time of 9.4 (95% CI 5.7, 13.2) minutes, whereas patients with a native papilla had shorter procedure times by 4.1 (95% 0.1, 8.0) minutes.Conclusion(s): In a large, multicenter database of pediatric ERCP procedures, we did not detect a significant difference in the rates of a successful procedure, adverse events, or procedure times between cases with and without trainee involvement. Future studies may evaluate if specific levels of involvement result in any significant effects on safety outcomes as educational opportunities continue to increase. Table 1Demographic Information

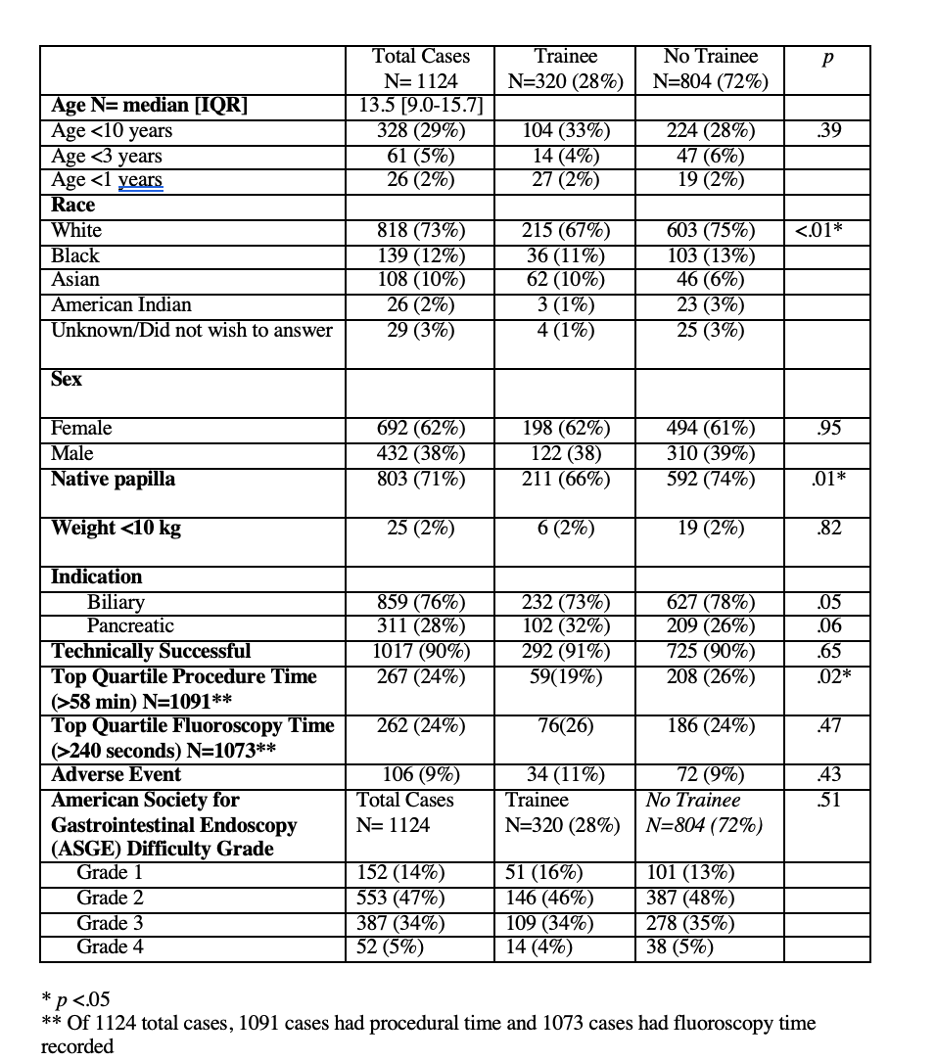 Demographic Information
Demographic Information