
Emergency Medicine: All Areas
Category: Abstract Submission
Emergency Medicine VII

Katie Dorney, MD, MHPEd
Associate fellowship director and Attending physician
Boston Children's Hospital
Newton, Massachusetts, United States
 Solid lines represent hospital-level, annual procalcitonin test utilization among pediatric patients aged 0-17 years seen in the emergency department from July 1, 2011 through June 30, 2020.
Solid lines represent hospital-level, annual procalcitonin test utilization among pediatric patients aged 0-17 years seen in the emergency department from July 1, 2011 through June 30, 2020.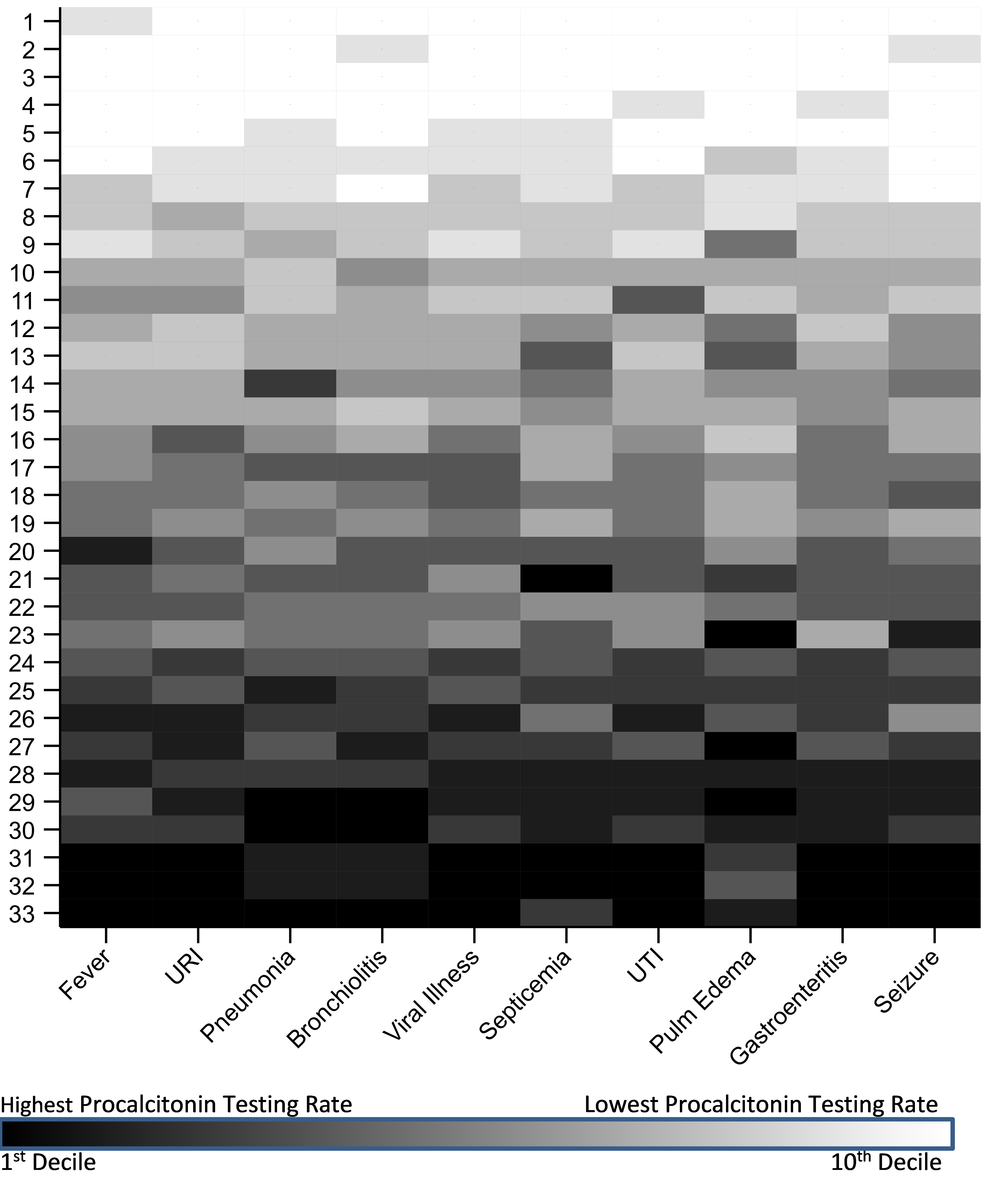 Hospital-level PCT testing for select APR-DRG diagnostic groups among pediatric patients treated in the ED from July 1 2016 through June 30 2020. For each diagnostic group, hospitals were ranked according to PCT testing rate and categorized into deciles. Hospitals were assigned an aggregate ranking. Thus, hospital 1 had the lowest aggregate PCT testing rate across the 10 diagnostic groups, and hospital 33 had the highest. URI = upper respiratory infection; UTI = urinary tract infection
Hospital-level PCT testing for select APR-DRG diagnostic groups among pediatric patients treated in the ED from July 1 2016 through June 30 2020. For each diagnostic group, hospitals were ranked according to PCT testing rate and categorized into deciles. Hospitals were assigned an aggregate ranking. Thus, hospital 1 had the lowest aggregate PCT testing rate across the 10 diagnostic groups, and hospital 33 had the highest. URI = upper respiratory infection; UTI = urinary tract infection