Cardiology
Category: Abstract Submission
Cardiology II

Abhishek Chakraborty, MD, FACC
Assistant Professor, Pediatric Cardiology
University of Tennessee Health Sciences
Memphis, Tennessee, United States
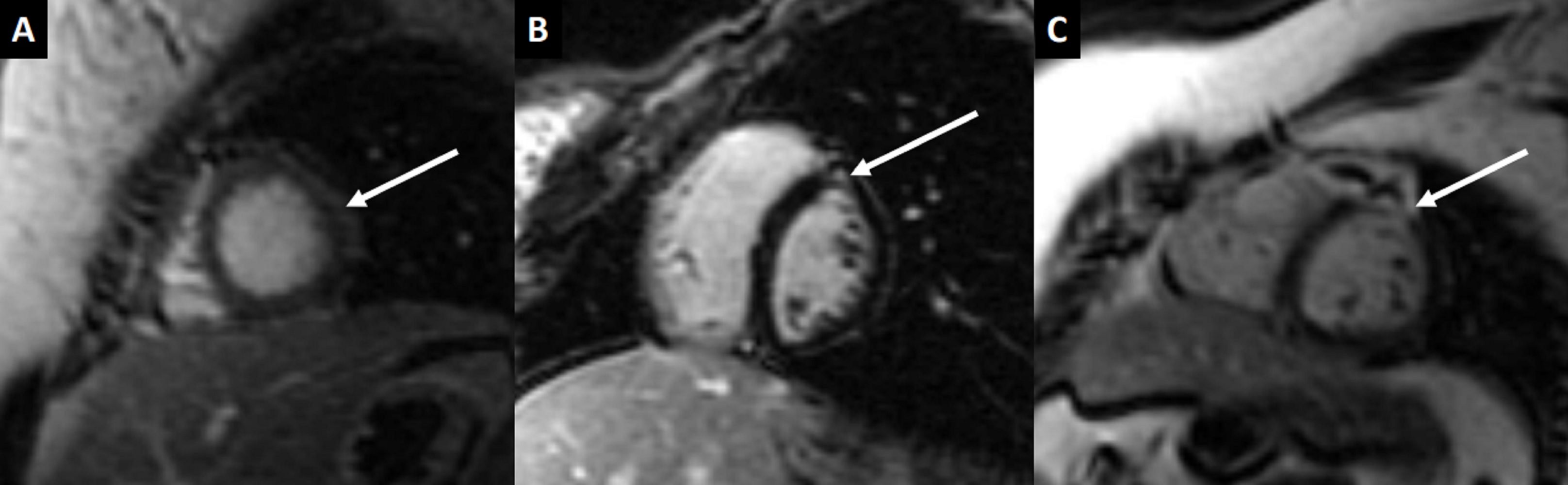 Figure 1. Cardiovascular magnetic resonance short axis late gadolinium enhancement in three separate patients. A. Patient 1. Apical segment with epicardial enhancement in the lateral wall (arrow). B. Patient 2. Mid segment with mid myocardial enhancement in the anteroseptal wall (arrow). C. Patient 3. Mid segment with epicardial enhancement in the anterior wall (arrow).
Figure 1. Cardiovascular magnetic resonance short axis late gadolinium enhancement in three separate patients. A. Patient 1. Apical segment with epicardial enhancement in the lateral wall (arrow). B. Patient 2. Mid segment with mid myocardial enhancement in the anteroseptal wall (arrow). C. Patient 3. Mid segment with epicardial enhancement in the anterior wall (arrow).