
Global Neonatal & Children's Health
Category: Abstract Submission
Global Child and Adolescent Health III
Nita Shrestha, MD
Fellow
John H Stroger Jr. Hospital of Cook County
Chicago, Illinois, United States
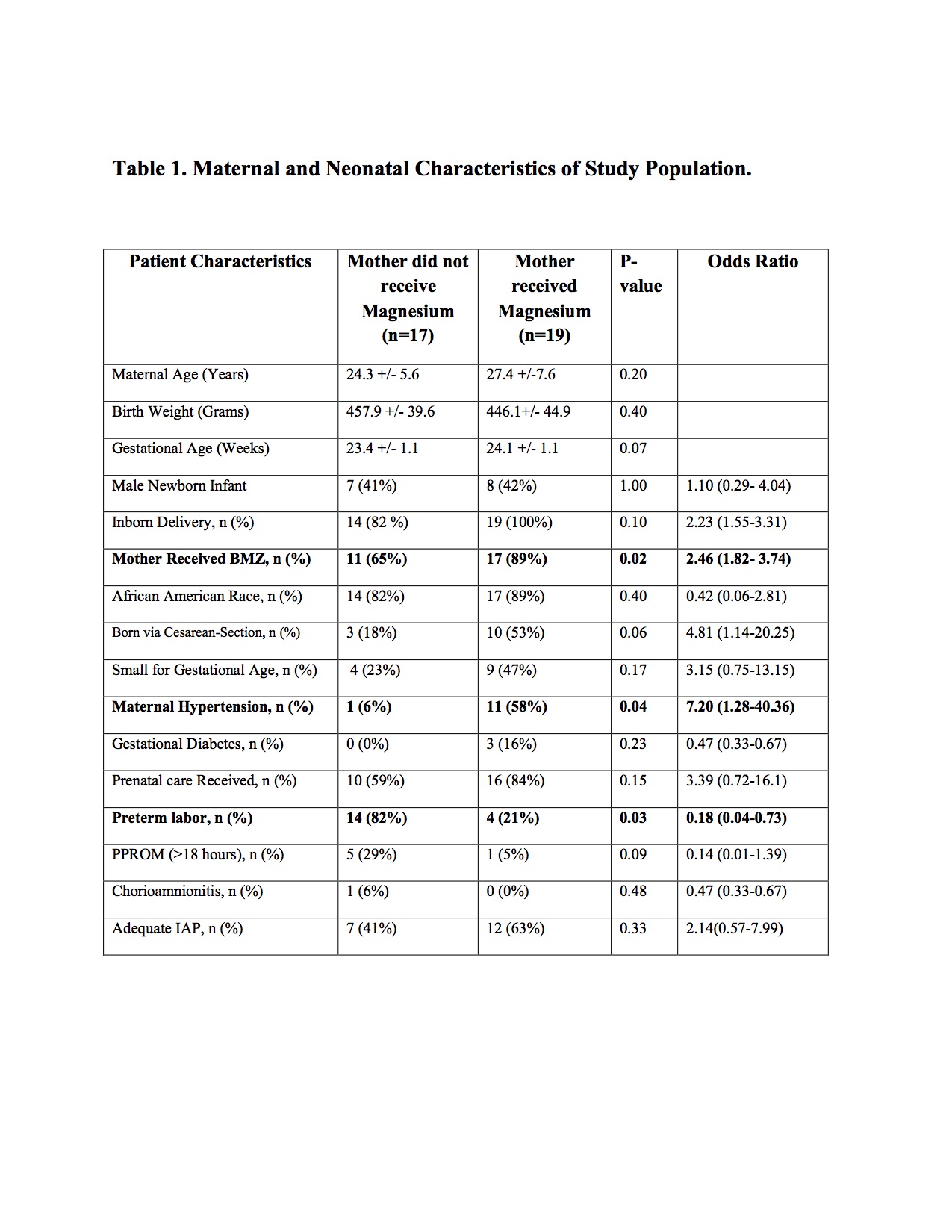 BMZ-Betamethasone; PPROM-Preterm Premature Rupture of Membrane, IAP-Intrapartum Antibiotic Prophylaxis
BMZ-Betamethasone; PPROM-Preterm Premature Rupture of Membrane, IAP-Intrapartum Antibiotic Prophylaxis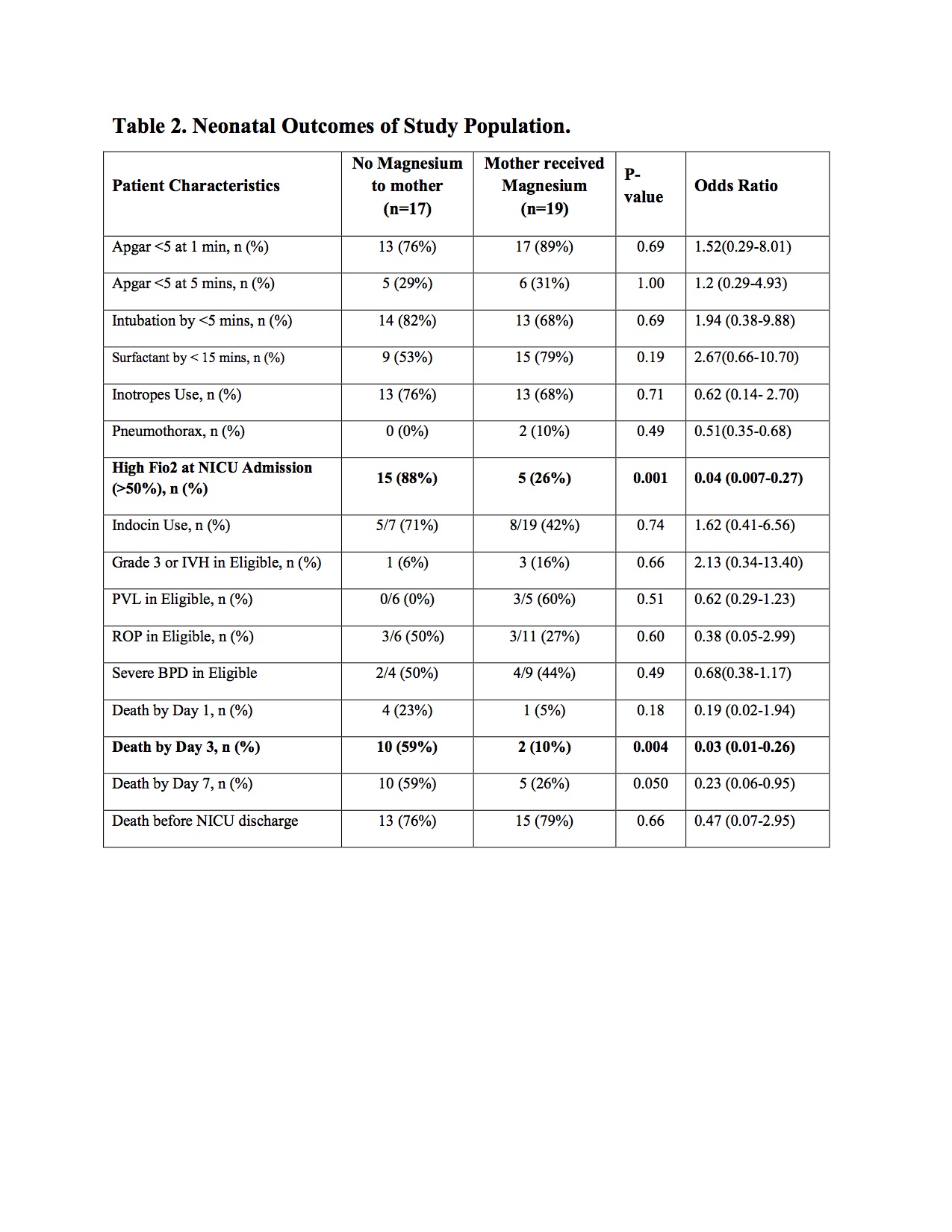 NICU- Neonatal Intensive Care Unit. P value < 0.05 is significant.
NICU- Neonatal Intensive Care Unit. P value < 0.05 is significant.