
Critical Care
Category: Abstract Submission
Critical Care III

Roman Gusdorf, BS
Medical Student
Vanderbilt University School of Medicine
Nashville, Tennessee, United States
 Demographics of patients in each cohort
Demographics of patients in each cohort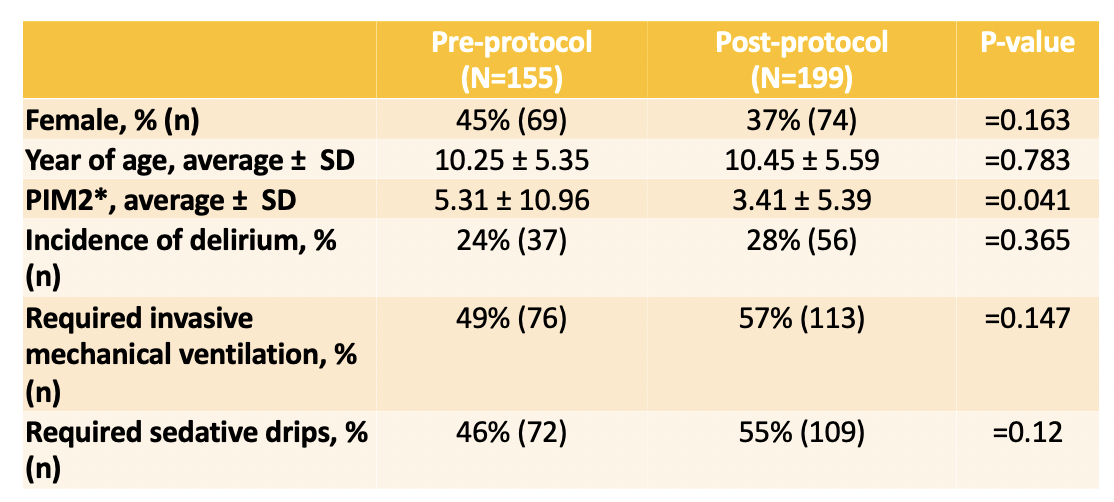 Demographic and clinical factors of patients in each cohort
Demographic and clinical factors of patients in each cohort