
Hospital Medicine: Hospital Medicine Quality Improvement
Category: Abstract Submission
Hospital Medicine: QI
 photo")
Jayme Wilder, MD (she/her/hers)
Hospitalist
Boston Children's Hospital
Boston, Massachusetts, United States
.png) Run chart depicting percent of direct admissions with I-PASS handoff document present in the EMR per month since implementation. Dashed line represents the median.
Run chart depicting percent of direct admissions with I-PASS handoff document present in the EMR per month since implementation. Dashed line represents the median.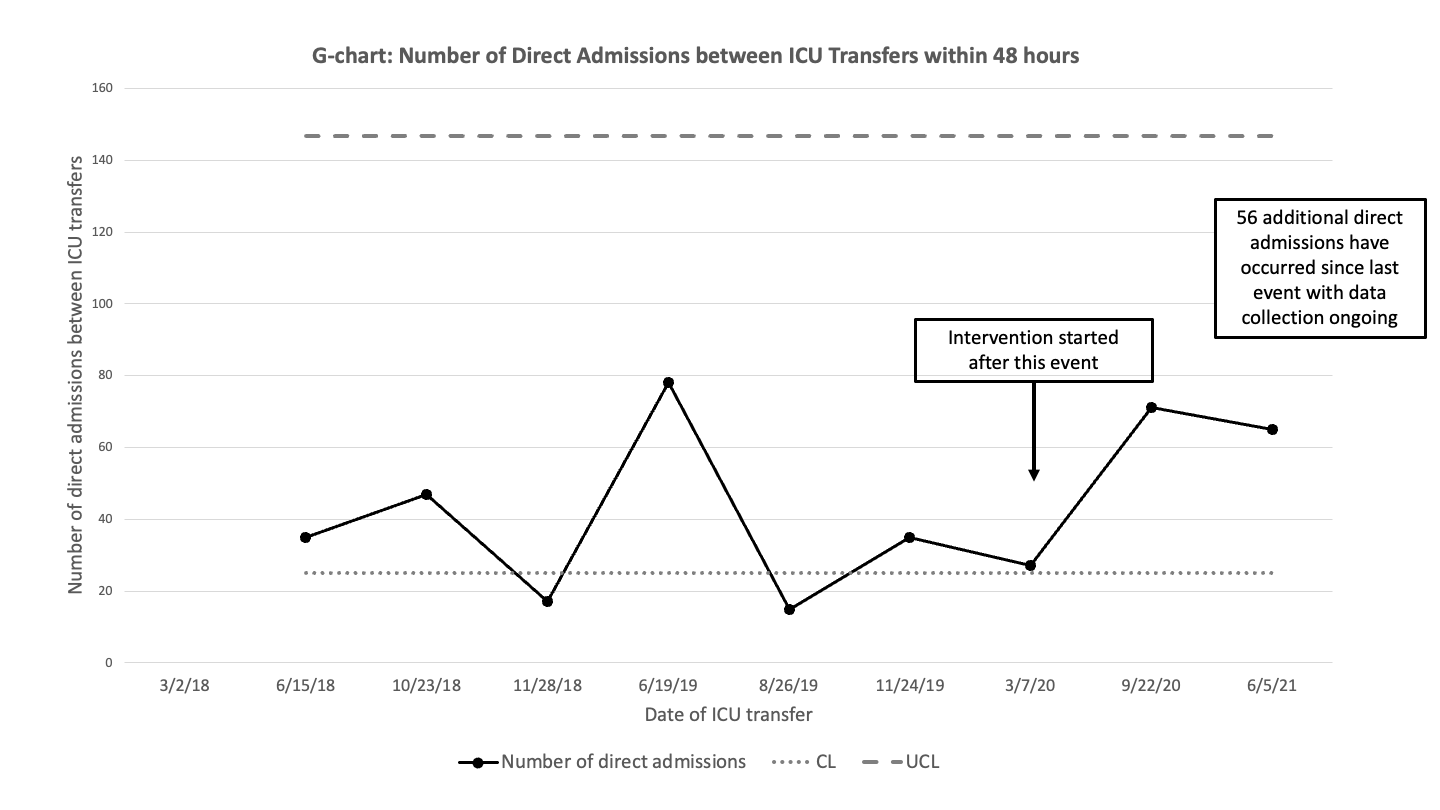 G-chart showing the number of direct admissions to the PHM service that were not transferred to ICU between direct admissions to the PHM service that were transferred to the ICU within 48 hours of admission. The upper control limit (dashed line) and center line (dotted line) are shown for the baseline.
G-chart showing the number of direct admissions to the PHM service that were not transferred to ICU between direct admissions to the PHM service that were transferred to the ICU within 48 hours of admission. The upper control limit (dashed line) and center line (dotted line) are shown for the baseline.