
Hospital Medicine: Clinical
Category: Abstract Submission
Hospital Medicine: Education/Research/QI Potpourri

Rachel R. Osborn, MD
Assistant Professor Pediatrics
Yale University School of Medicine
New Haven, Connecticut, United States
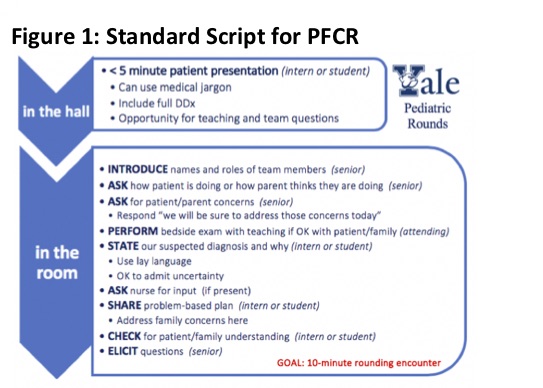 This card guided physician team communication with family. "In the room" had nearly identical wording in the pre and post intervention periods, excepting a substitution of "state our suspected diagnosis and why" in place of "present the history and assessment."
This card guided physician team communication with family. "In the room" had nearly identical wording in the pre and post intervention periods, excepting a substitution of "state our suspected diagnosis and why" in place of "present the history and assessment."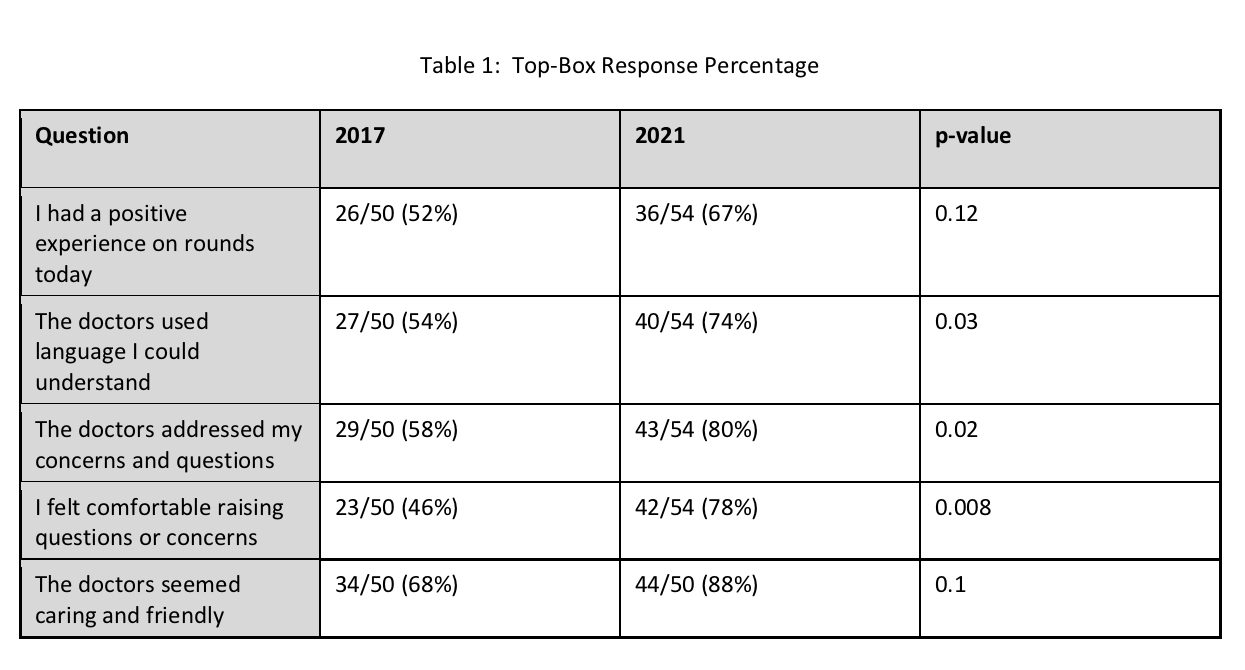 Proportion of responses in the "strongly agree" category acrosss all 5 Likert questions is shown here
Proportion of responses in the "strongly agree" category acrosss all 5 Likert questions is shown here