
Adolescent Medicine: Disordered Eating
Category: Abstract Submission
Adolescent Medicine III
 photo")
Jessica A. Lin, MD (she/her/hers)
Assistant Professor
Cincinnati Children's Hospital Medical Center
Cincinnati, Ohio, United States
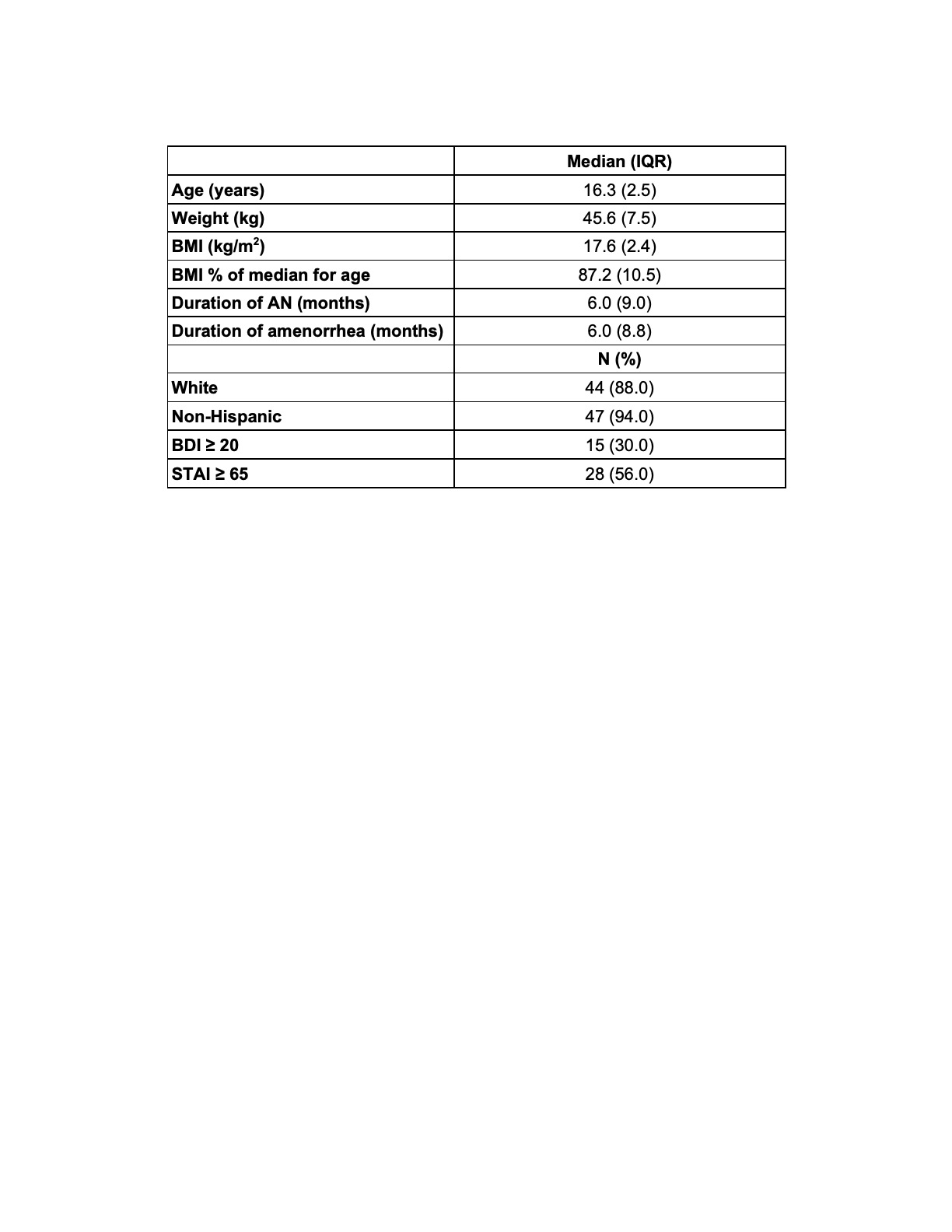 Note. IQR = interquartile range; BMI = body mass index; AN = anorexia nervosa;
Note. IQR = interquartile range; BMI = body mass index; AN = anorexia nervosa; 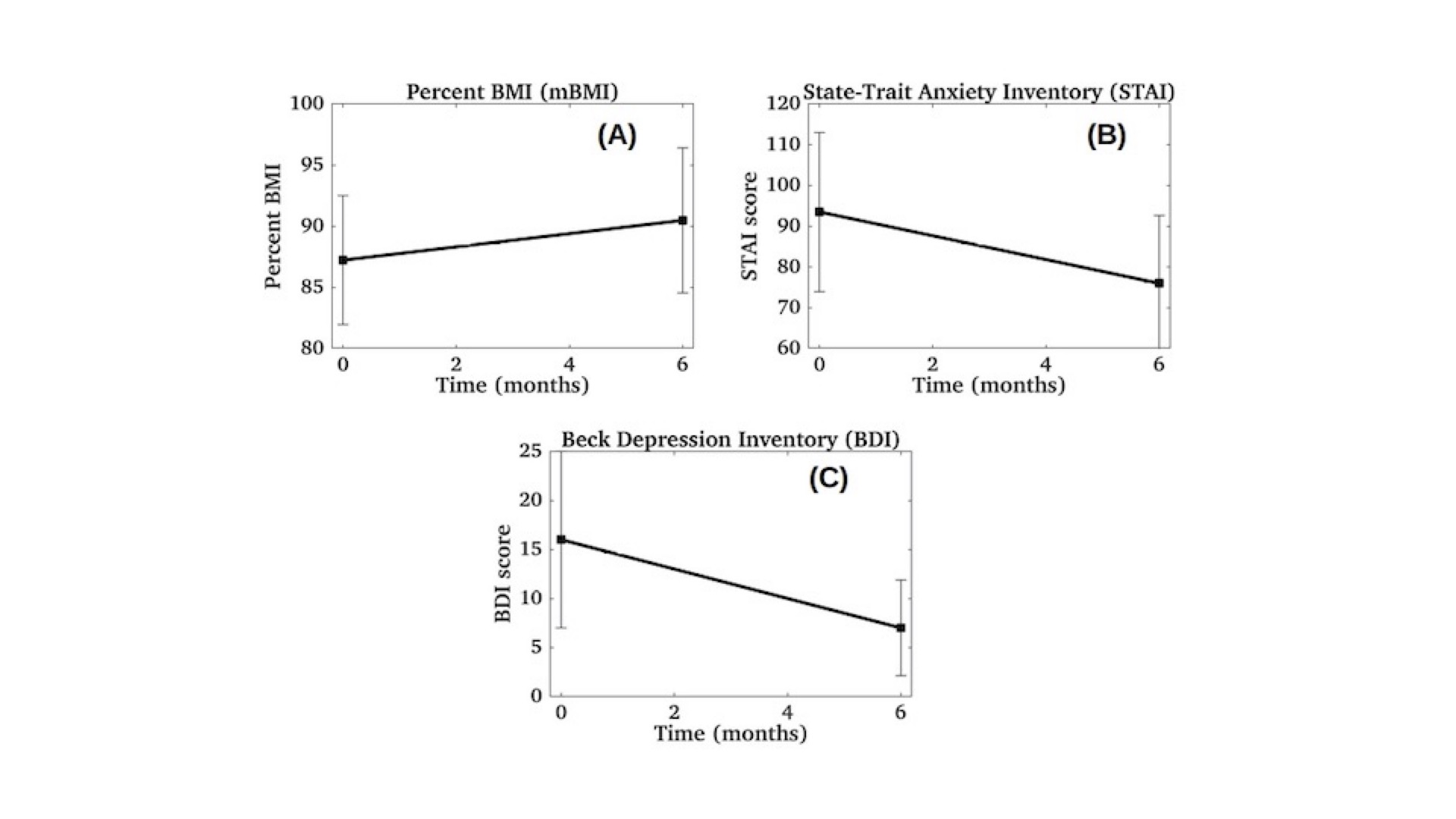 Fig. 2A = Change in percentage of median BMI (p < 0.01)
Fig. 2A = Change in percentage of median BMI (p < 0.01)