
Health Services Research
Category: Abstract Submission
Health Services Research III
 photo")
Jessica Campanile, BA (she/they)
Medical Student
Perelman School of Medicine at the University of Pennsylvania
Philadelphia, Pennsylvania, United States
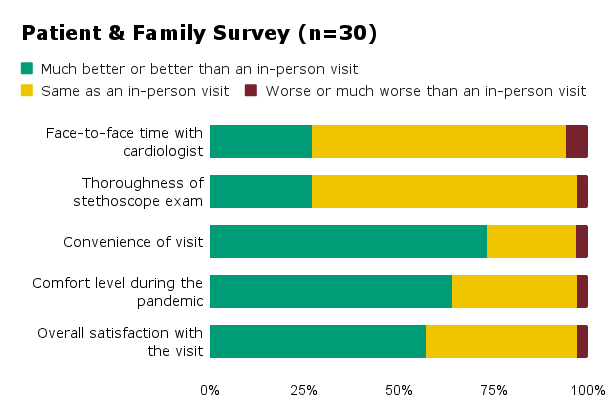 Patients and families (n=30) rated remote auscultation visit metrics compared to an in-person visit.
Patients and families (n=30) rated remote auscultation visit metrics compared to an in-person visit.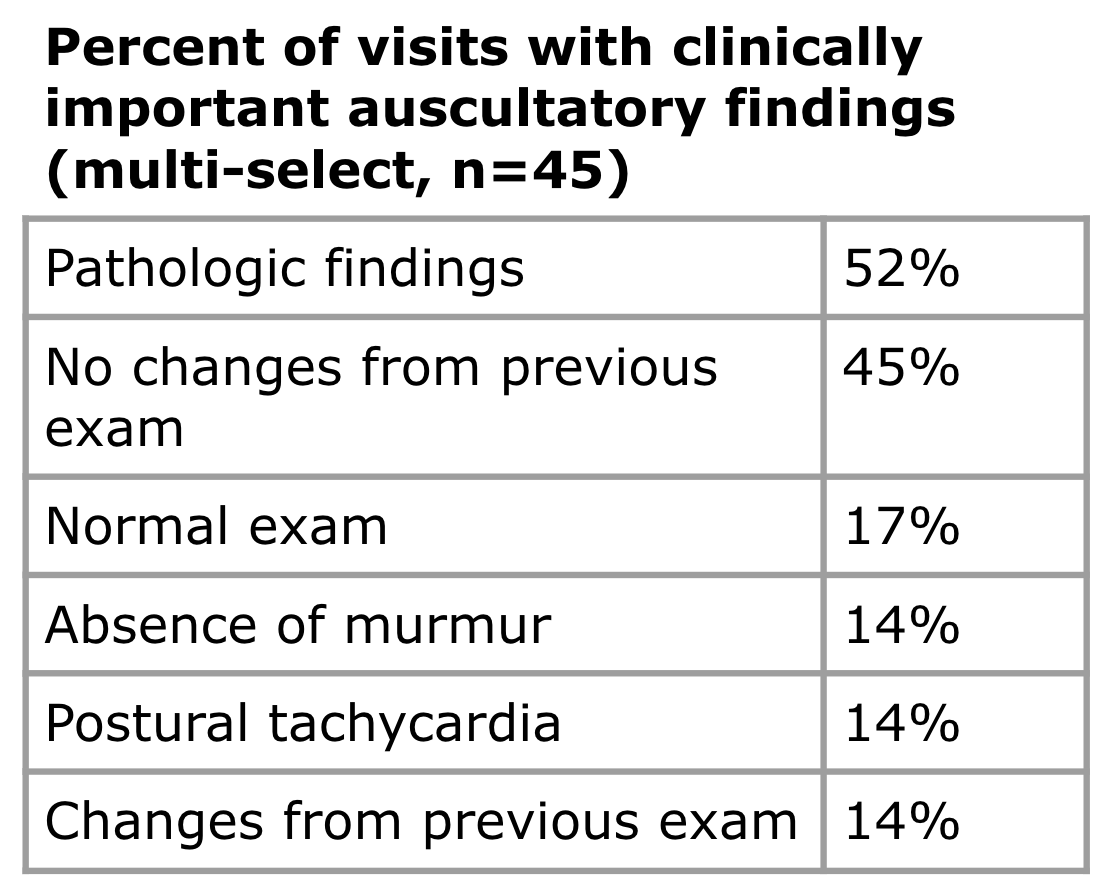 Percentage of visits (n=45) with selected clinically important findings according to cardiologist post visit survey is shown.
Percentage of visits (n=45) with selected clinically important findings according to cardiologist post visit survey is shown.