
Hospital Medicine: Clinical
Category: Abstract Submission
Hospital Medicine: Clinical NOS

Maheshwor Kafle, MD
Attending Hospitalist
Phoenix Children's Hospital
Phoenix, Arizona, United States
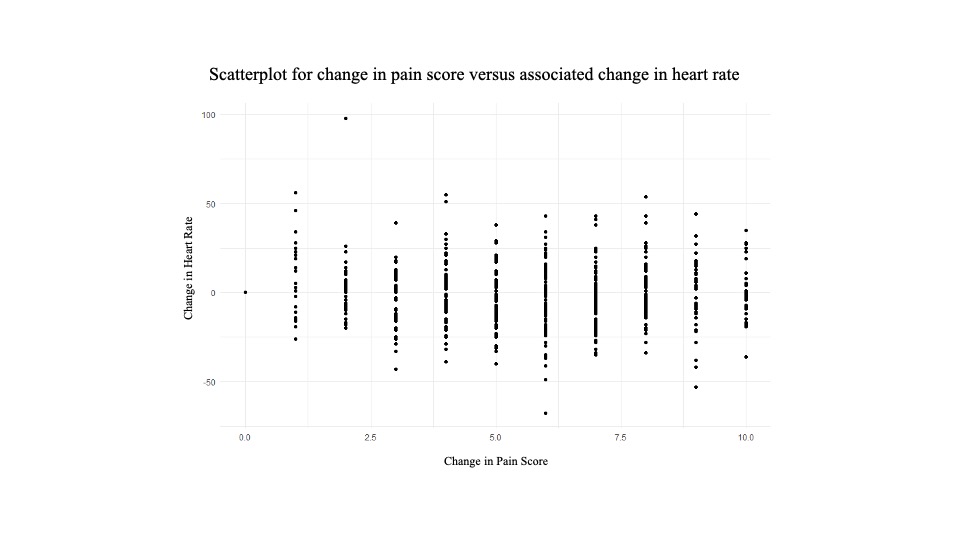 Each point represents an individual patient. Highest and lowest pain score values (among ten total recorded values) for each patient were used to calculate the change in pain score. Associated HRs within one-hour of these pain score values were used to calculate the corresponding change in HR.
Each point represents an individual patient. Highest and lowest pain score values (among ten total recorded values) for each patient were used to calculate the change in pain score. Associated HRs within one-hour of these pain score values were used to calculate the corresponding change in HR..jpg) Each point represents an individual patient. Highest and lowest pain score values (among ten total recorded values) for each patient were used to calculate the change in pain score. Associated SBPs and DBPs within one-hour of these pain score values were used to calculate the corresponding changes in blood pressure.
Each point represents an individual patient. Highest and lowest pain score values (among ten total recorded values) for each patient were used to calculate the change in pain score. Associated SBPs and DBPs within one-hour of these pain score values were used to calculate the corresponding changes in blood pressure.