379 - Utility of Urine Testing for the Detection of Asymptomatic Urinary Tract Infections in Pediatric
Patients with Cancer: A retrospective chart review
Saturday, April 23, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 379 Publication Number: 379.206
Rasha D. Sawaya, American University of Beirut, Dublin, Dublin, Ireland; Ola El Kebbi, American University of Beirut, Beirut, Beyrouth, Lebanon; Dima A. Hamideh, american university of beirut, Hamra, Beyrouth, Lebanon; Mohamed Radwan, The Children's Hospital at Monmouth Medical Center, Long Branch, NJ, United States; Hashem Nassereddine, American University of Beirut, Dearborn, MI, United States; Adonis Wazir, American University of Beirut Medical Center, London, England, United Kingdom; Sarah Abdul Nabi, American University of Beirut Medical Center, Beirut, Beyrouth, Lebanon; Osama K. Ibrahim, Hasbro Children's Hospital at Rhode Island Hospital, providence, RI, United States; Maha Makki, American University of Beirut, Beirut, Beyrouth, Lebanon
Background: The frequency of urinary tract infections in febrile children with cancer has not been extensively studied. While a CBC and blood culture are standard tests for all febrile children with cancer on chemotherapy, urine testing remains controversial. In our institutional guidelines, we obtain urine studies on all febrile children with cancer.
Objective: We aimed to determine the utility of urine cultures in asymptomatic febrile children with cancer as well as the diagnostic performance of the UA.
Design/Methods: This is a single centre, retrospective chart review, of all asymptomatic febrile pediatric patients with cancer, 1 month to 18 years old, presenting to the Emergency or Outpatient Department from 01/01/2014 to 12/31/2018 who had a urine culture obtained at presentation. Fever was defined as a single oral temperature ≥38.3°C or ≥38°C for more than an hour or 2 elevations ≥38°C in a 12-hour period. Asymptomatic was defined as none of the following urinary symptoms present: hematuria, dysuria, frequency, suprapubic, inguinal or costovertebral pain or tenderness. To avoid repetitive bias, we selected one random febrile visit per patient. Patients were analyzed into 2 groups: urine culture positive (POS) (defined as at least 1 organism growth ≥ 100,000 cfu) and urine culture negative (NEG). Descriptive analysis and sensitivity and specificity analysis were done on STATA MP. P-value < 0.05 was considered statistically significant.
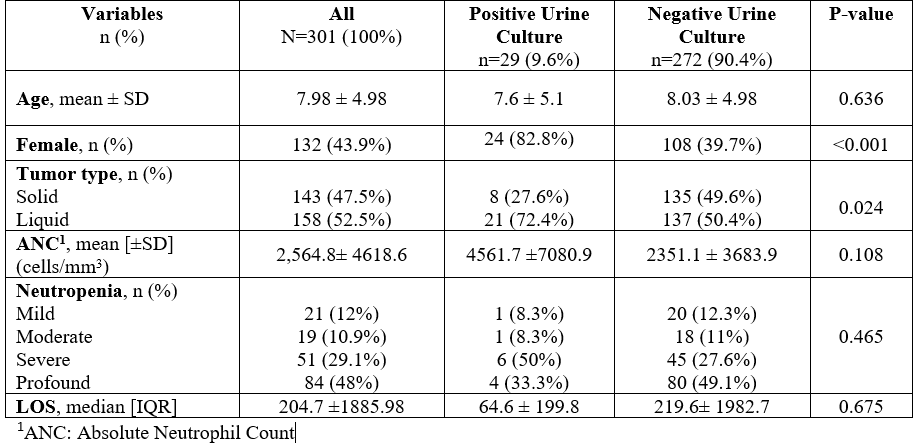
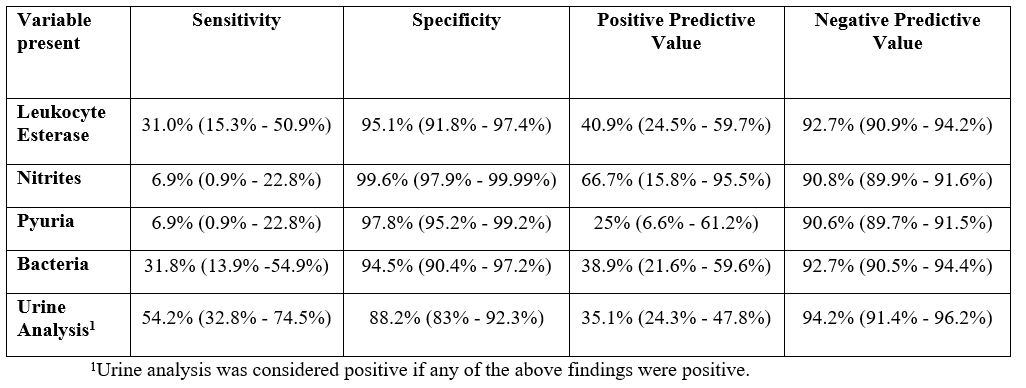
Results: 664 charts were reviewed, and 301 unique patient visits included, where the majority (56%) were male, with a mean age of 8 years±5. 9.6% had a positive urine culture. Predictors of a positive urine culture included female gender (82.8% POS VS 39.7% NEG, p< 0.001), liquid tumors (72.4% POS vs 50.4% NEG, p=0.024) and a positive UA (defined as any positive variable within) at presentation (54.2% POS VS 11.8% NEG, p< 0.001). See Table 1. Performance of the UA in predicting a positive urine culture: sensitivity=54.2% (32.8%-74.5%), specificity=88.2% (83%-92.3%), PPV=35.1% (24.3%-47.8%) and NPV=94.2% (91.4%-96.2%). See table 2. These results were similar in the neutropenic subgroup.Conclusion(s): The rates of a positive urine culture in febrile children with cancer is not insignificant (9.6%) and therefore we recommend urine testing in all febrile children with cancer, irrespective of their symptoms. The interpretation of the urinalysis should still be done with caution and further studies looking at the outcomes of these patients is needed. Characteristics of all patients with positive and negative urine cultures Diagnostic Performance of Urine Analysis

.jpg "Rasha D. Sawaya, MD photo")