
Neonatal Neurology: Clinical
Category: Abstract Submission
Neurology 7: Neonatal Neurology Term Imaging
 photo")
Chelsea Munster, BA (she/her/hers)
Clinical Research Assistant
Brigham and Women's Hospital
731 South Eureka St, California, United States
.png) Abbreviations: NE, neonatal encephalopathy; UA, umbilical artery; UV, umbilical venous; BD, base deficit
Abbreviations: NE, neonatal encephalopathy; UA, umbilical artery; UV, umbilical venous; BD, base deficit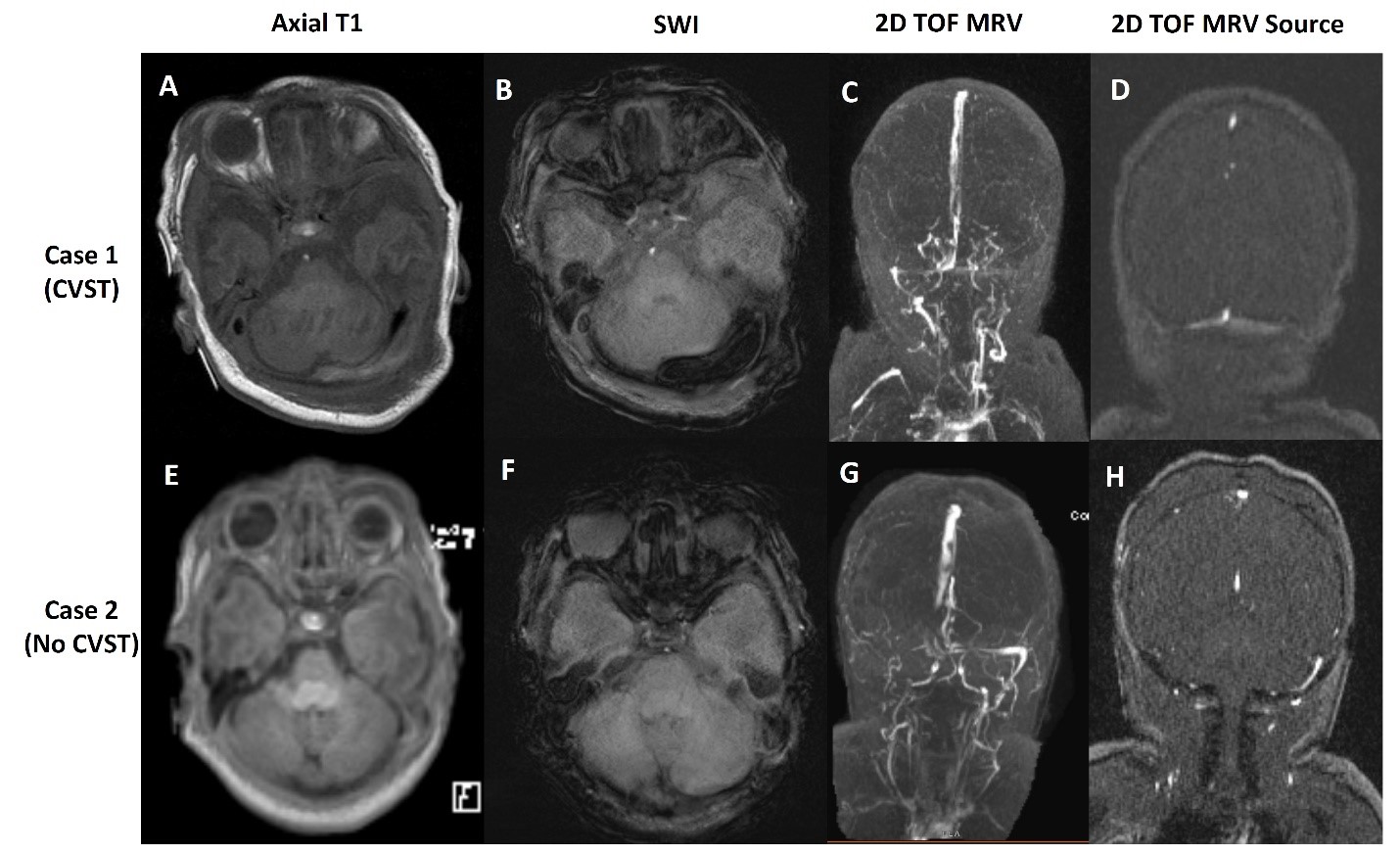 Case 1: Demonstration of linear hyperintensity on Axial T1(A) and susceptibility on SWI (B) in the region of the left transverse sinus not associated with significant asymmetry on MRV (C and D)
Case 1: Demonstration of linear hyperintensity on Axial T1(A) and susceptibility on SWI (B) in the region of the left transverse sinus not associated with significant asymmetry on MRV (C and D)