
Health Equity/Social Determinants of Health
Category: Abstract Submission
Health Equity/Social Determinants of Health IV
Gauthami Soma, MD
Fellow in Pediatric Emergency Medicine
Yale School of Medicine
West Hartford, Connecticut, United States
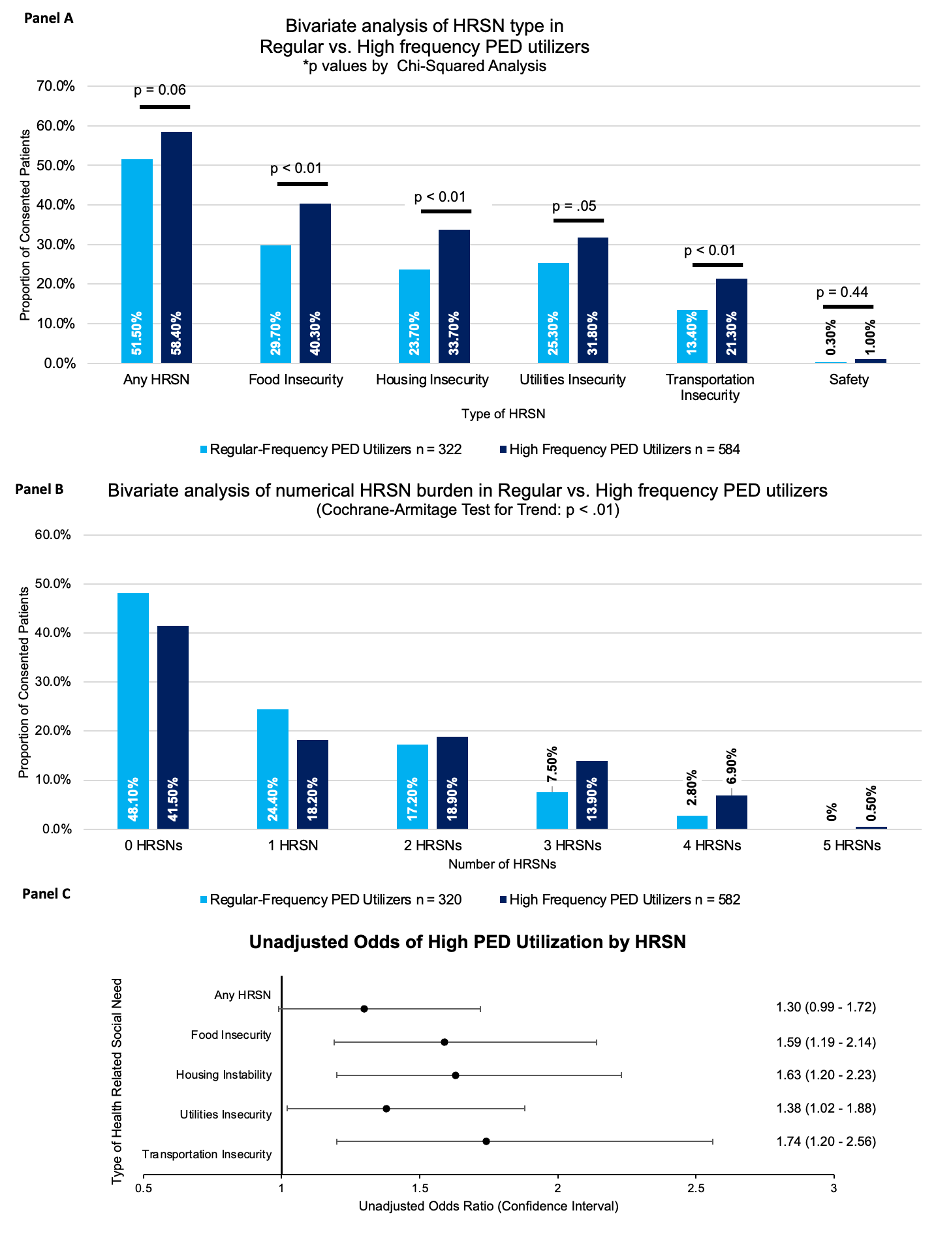 1. Panel A: Bivariate analysis of HRSN type in Regular vs. High-frequency PED utilizes. P-values by chi-squared analysis.
1. Panel A: Bivariate analysis of HRSN type in Regular vs. High-frequency PED utilizes. P-values by chi-squared analysis.