
Neonatal Infectious Diseases/Immunology
Category: Abstract Submission
Neonatal Infectious Diseases/Immunology: COVID-19
 photo")
Daniele De Luca, MD, PhD (he/him/his)
Full Professor
APHP-Paris Saclay University
Paris, Ile-de-France, France
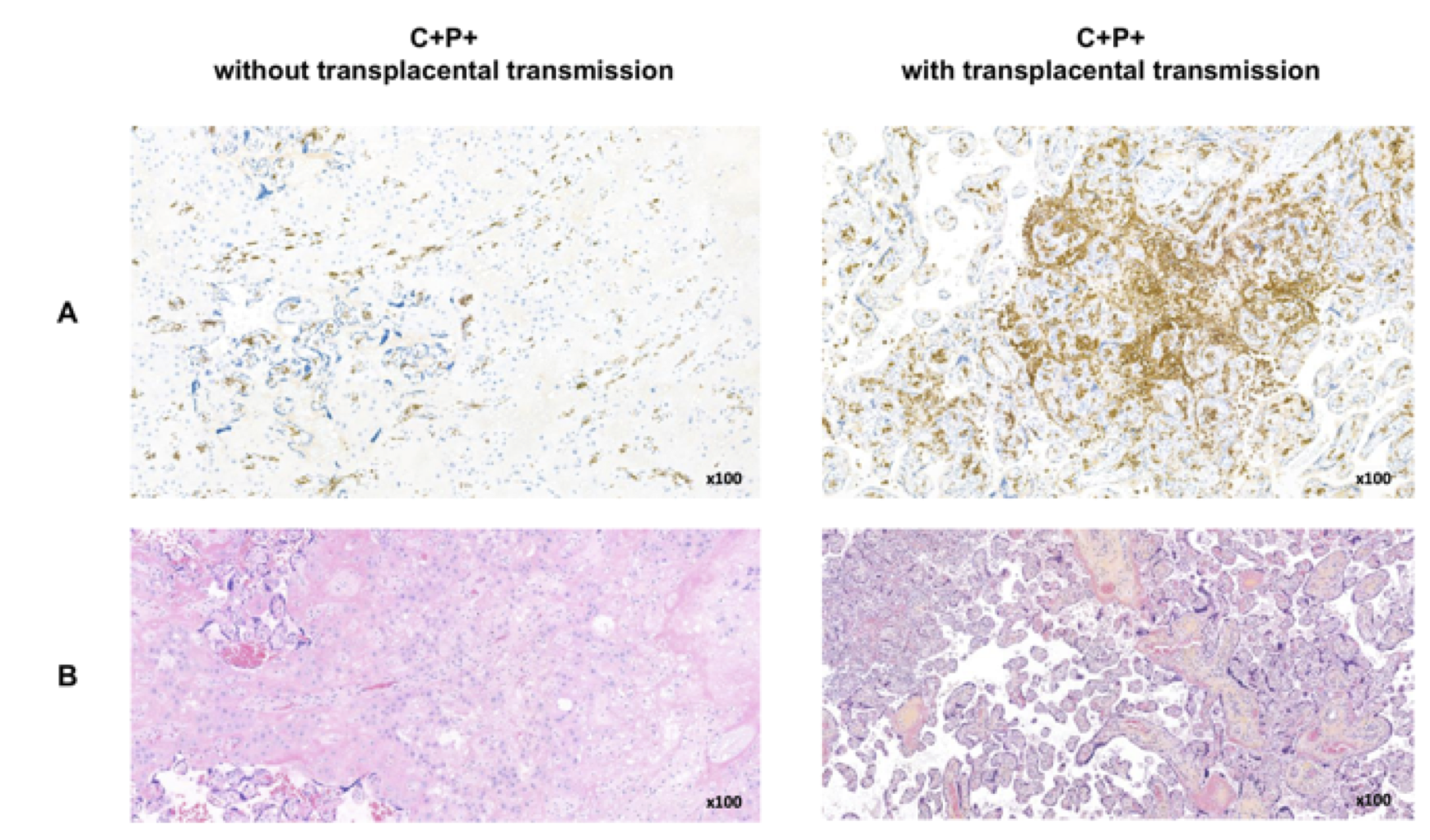 Images from a pregnancy without (left) or with transplacental transmission (right) are shown. Panels A and B depict CD163 immunostaining and HES stain, respectively. Infected placenta with transplacental transmission shows a higher degree of chronic intervillositis as seen in HES stain with macrophage infiltration as demonstrated by CD163 immunostaining.
Images from a pregnancy without (left) or with transplacental transmission (right) are shown. Panels A and B depict CD163 immunostaining and HES stain, respectively. Infected placenta with transplacental transmission shows a higher degree of chronic intervillositis as seen in HES stain with macrophage infiltration as demonstrated by CD163 immunostaining.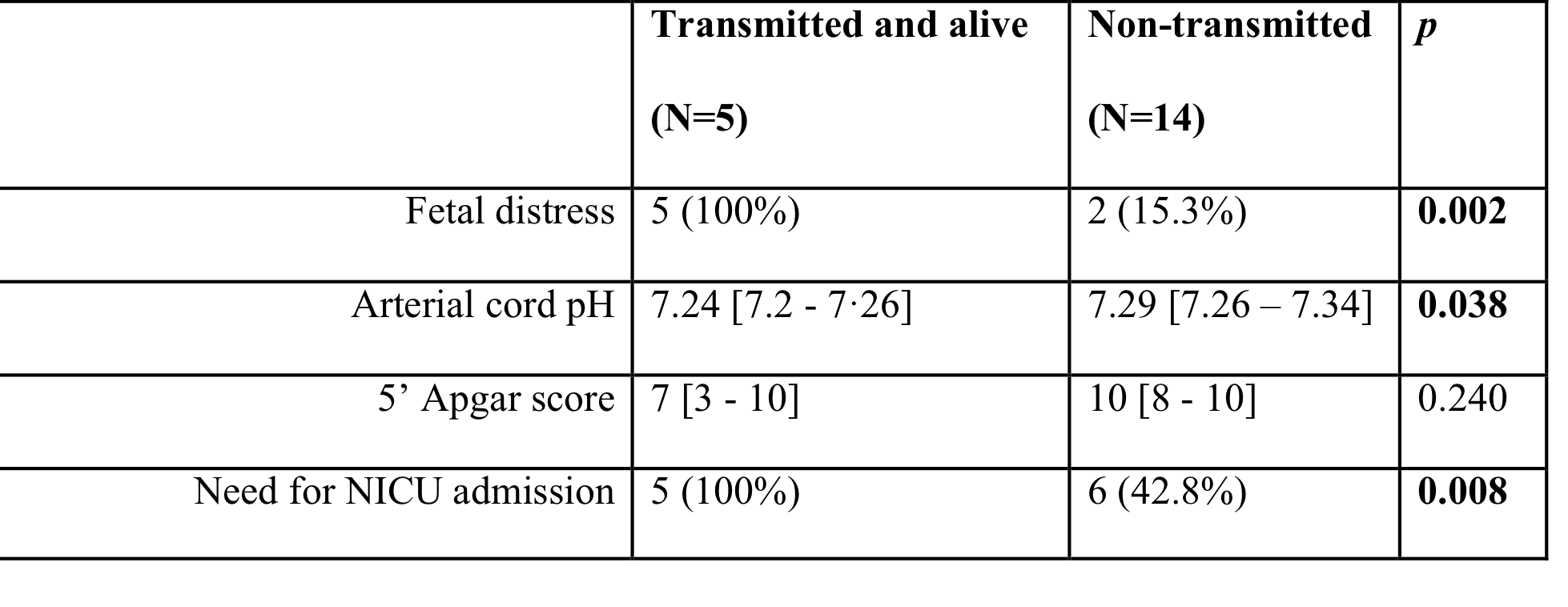 Live neonates with transplacentally transmitted SARS-CoV-2 infection were compared to 14 neonates born from women with COVID-19 during the third trimester. Data are expressed as median [25th – 75th percentile] or number (%). Abbreviations: NICU: neonatal intensive care unit.
Live neonates with transplacentally transmitted SARS-CoV-2 infection were compared to 14 neonates born from women with COVID-19 during the third trimester. Data are expressed as median [25th – 75th percentile] or number (%). Abbreviations: NICU: neonatal intensive care unit.