
Neonatal Fetal Nutrition & Metabolism
Category: Abstract Submission
Neonatal Fetal Nutrition & Metabolism II

Stephanie S. Chassen, MD
Assistant Professor of Pediatrics
University of Colorado Neonatology
Aurora, Colorado, United States
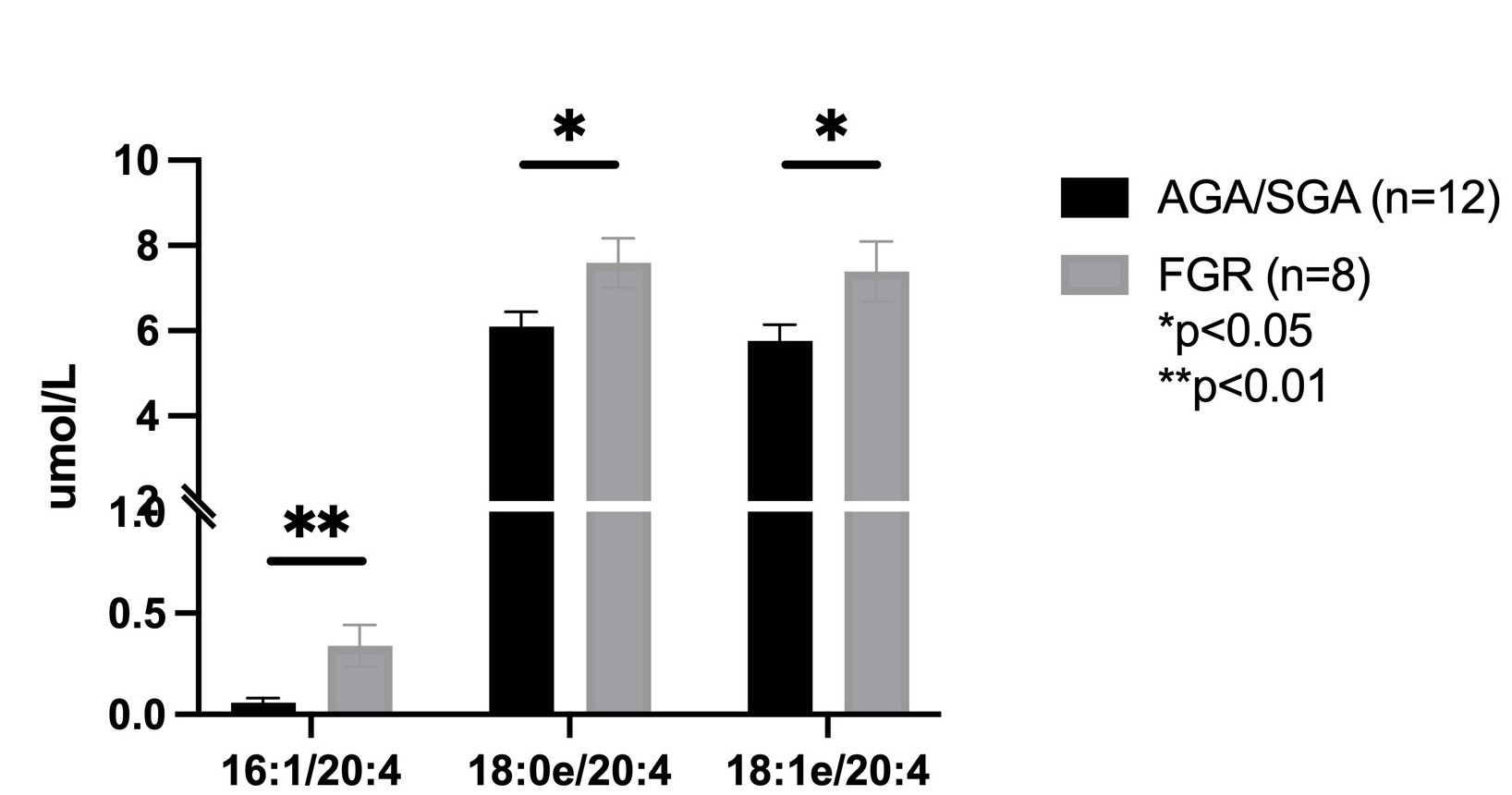 Graph depicting significantly increased concentrations (umol/L) of the phosphatidylcholine (PC) molecules containing 20:4 (arachidonic acid) in cord plasma from fetal growth restricted (FGR) pregnancies.
Graph depicting significantly increased concentrations (umol/L) of the phosphatidylcholine (PC) molecules containing 20:4 (arachidonic acid) in cord plasma from fetal growth restricted (FGR) pregnancies.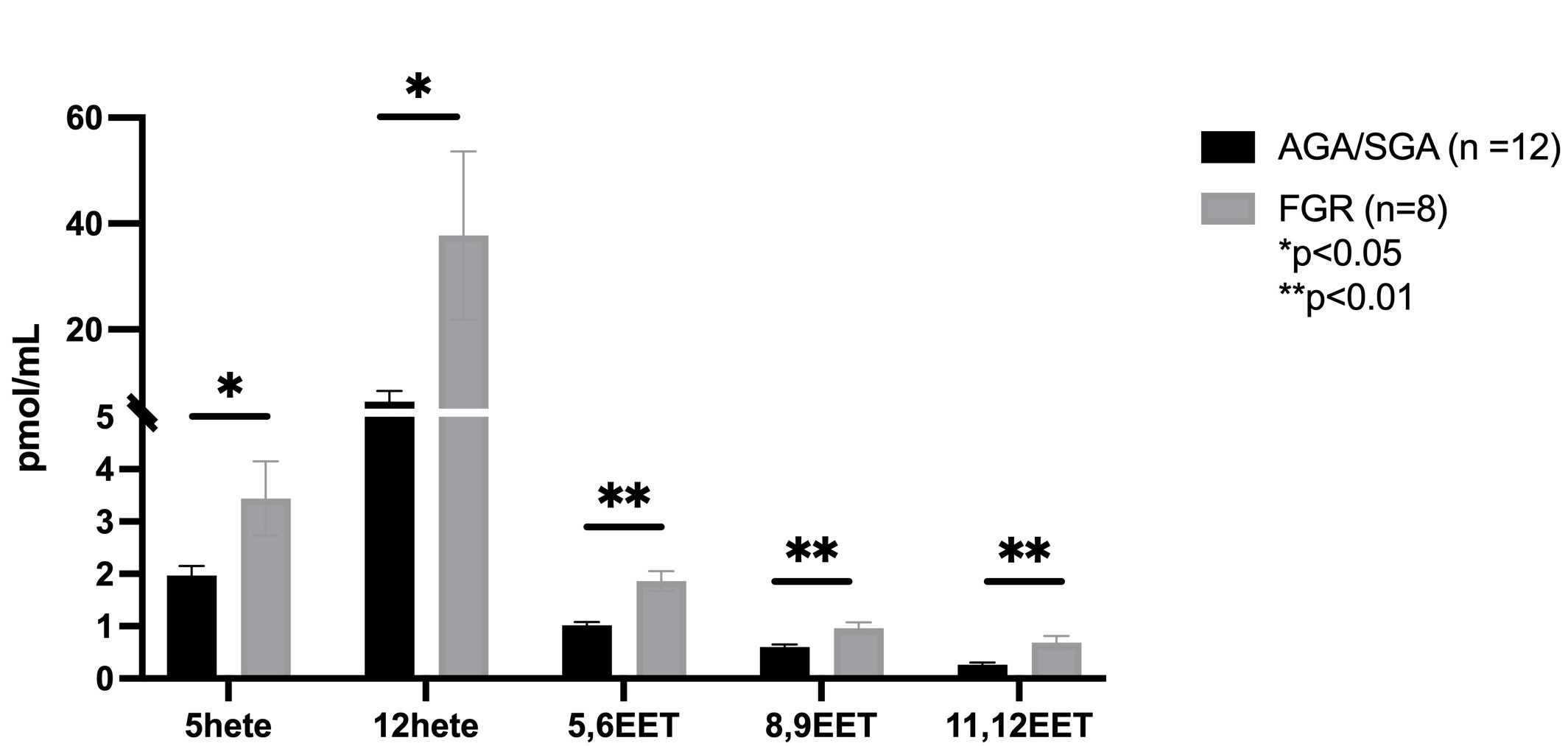 Graph depicting significantly increased concentrations (pmol/mL) of several eicosanoid molecules (epoxyeicosatrienoic acids, EETs; hydroxyeicosatetraenoic acids, Hetes) in cord plasma from fetal growth restricted (FGR) pregnancies.
Graph depicting significantly increased concentrations (pmol/mL) of several eicosanoid molecules (epoxyeicosatrienoic acids, EETs; hydroxyeicosatetraenoic acids, Hetes) in cord plasma from fetal growth restricted (FGR) pregnancies.