
Global Neonatal & Children's Health
Category: Abstract Submission
Global Child and Adolescent Health I
Elizabeth M. Keating, MD, MSPH (she/her/hers)
Assistant Professor
University of Utah
Salt Lake City, Utah, United States
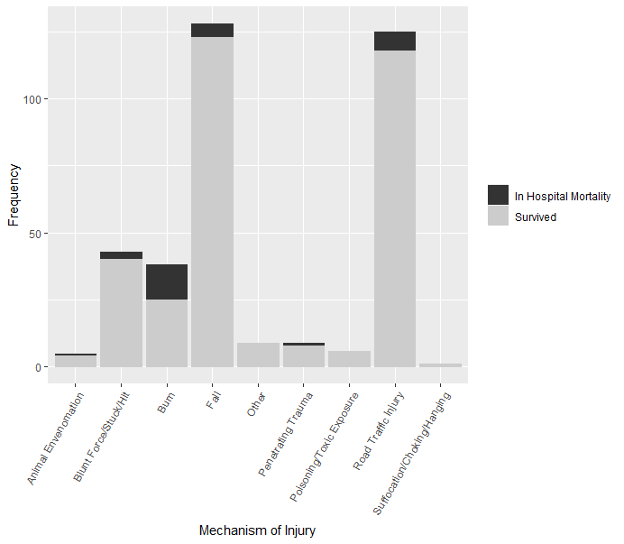 Bar plot of primary mechanisms of injury for pediatric injury patients with bars proportional to percentage of patients who survived and died.
Bar plot of primary mechanisms of injury for pediatric injury patients with bars proportional to percentage of patients who survived and died.