
Neonatal General
Category: Abstract Submission
Neonatology General 6: NOWS - Maternal-Fetal Exposures

Deepika Sankaran, MD
Neonatologist
University of California Davis Children's Hospital
Sacramento, California, United States
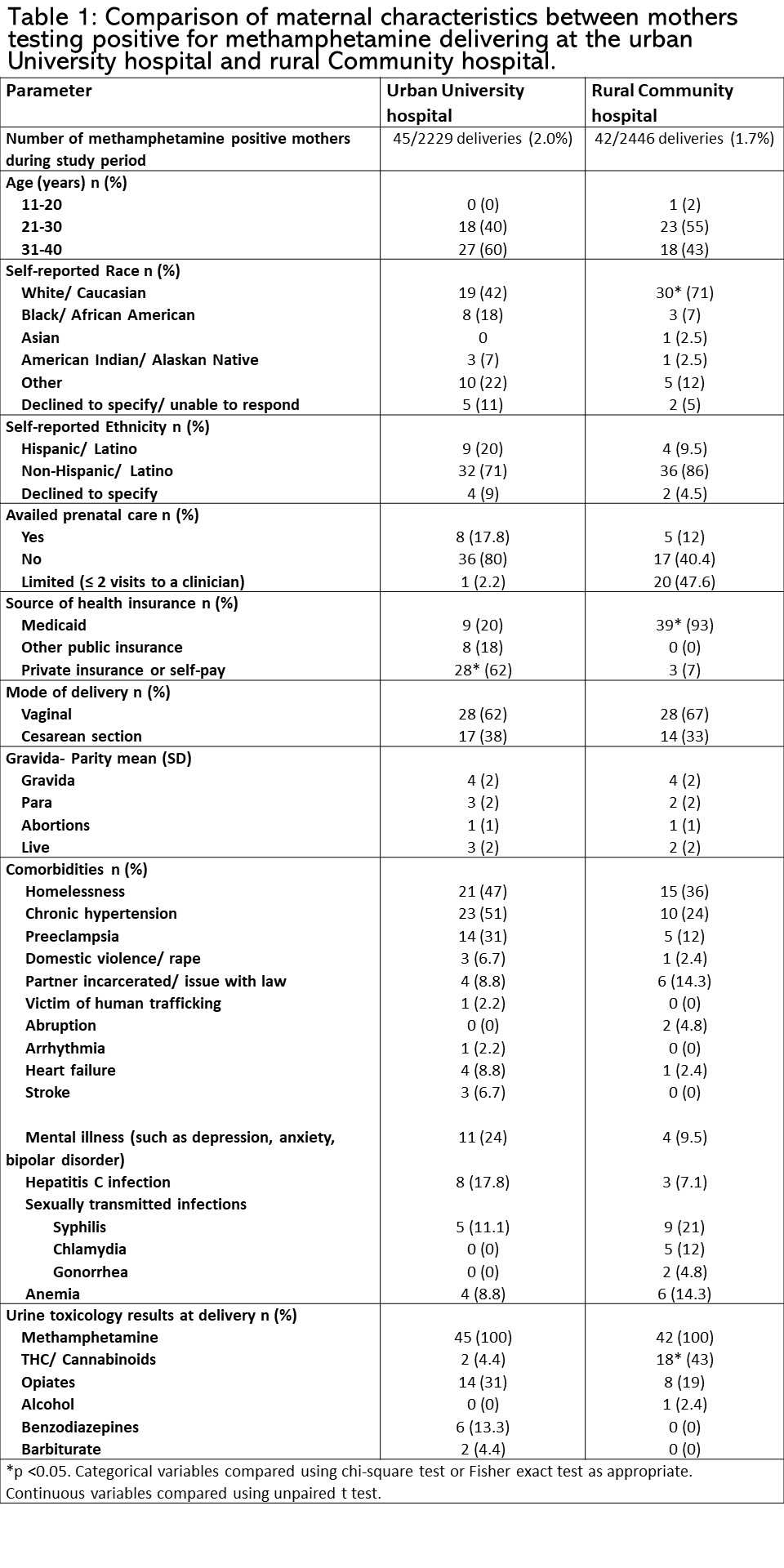 *p < 0.05. Categorical variables compared using chi-square test or Fisher exact test as appropriate. Continuous variables compared using unpaired t test.
*p < 0.05. Categorical variables compared using chi-square test or Fisher exact test as appropriate. Continuous variables compared using unpaired t test.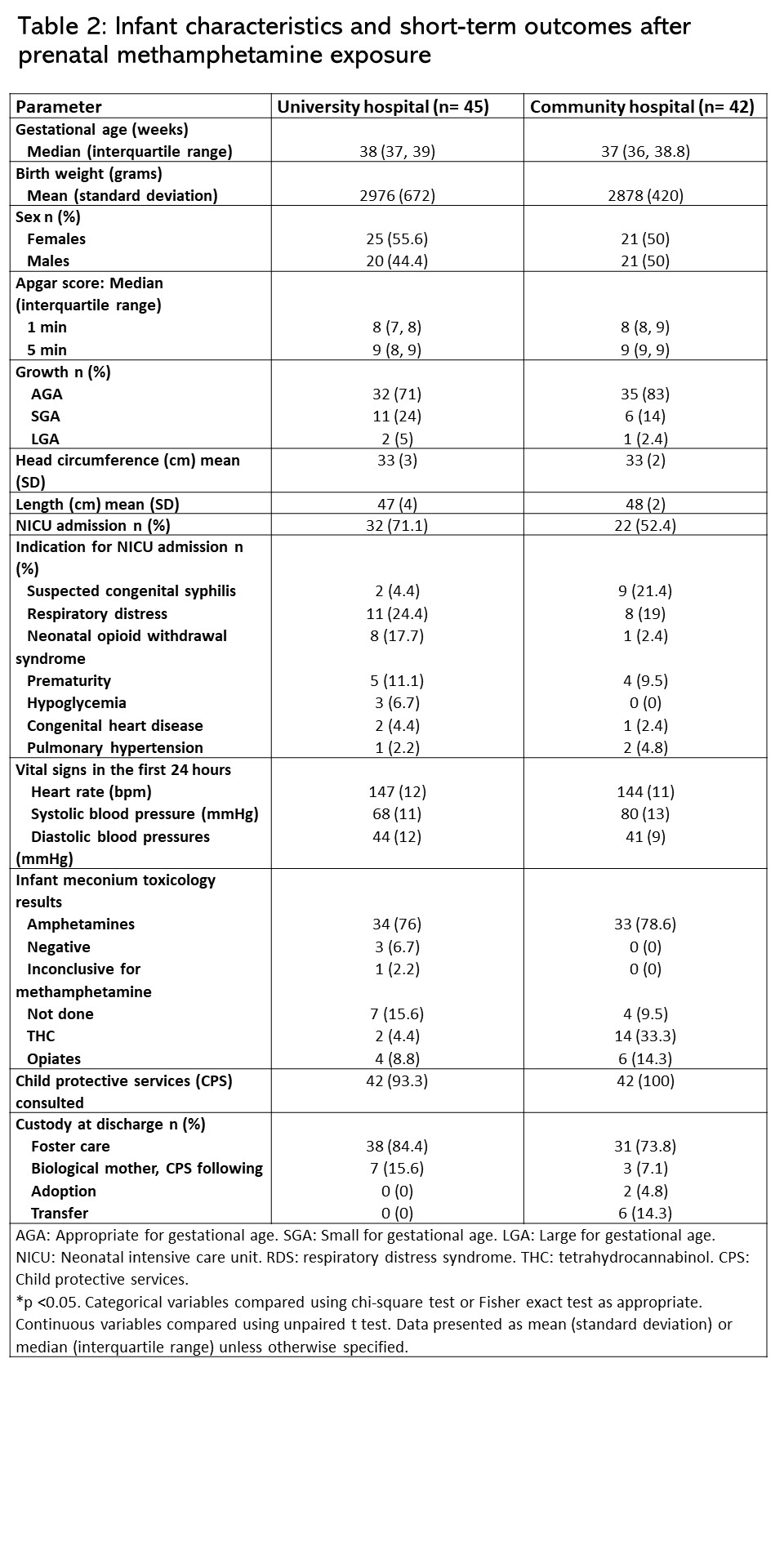 AGA: Appropriate for gestational age. SGA: Small for gestational age. LGA: Large for gestational age. NICU: Neonatal intensive care unit. RDS: respiratory distress syndrome. THC: tetrahydrocannabinol. CPS: Child protective services.
AGA: Appropriate for gestational age. SGA: Small for gestational age. LGA: Large for gestational age. NICU: Neonatal intensive care unit. RDS: respiratory distress syndrome. THC: tetrahydrocannabinol. CPS: Child protective services.