
Neonatal/Infant Resuscitation
Category: Abstract Submission
Neonatal/Infant Resuscitation II
 photo")
Vivek Shukla, MD (he/him/his)
Assistant Professor
University of Alabama at Birmingham
Birmingham, Alabama, United States
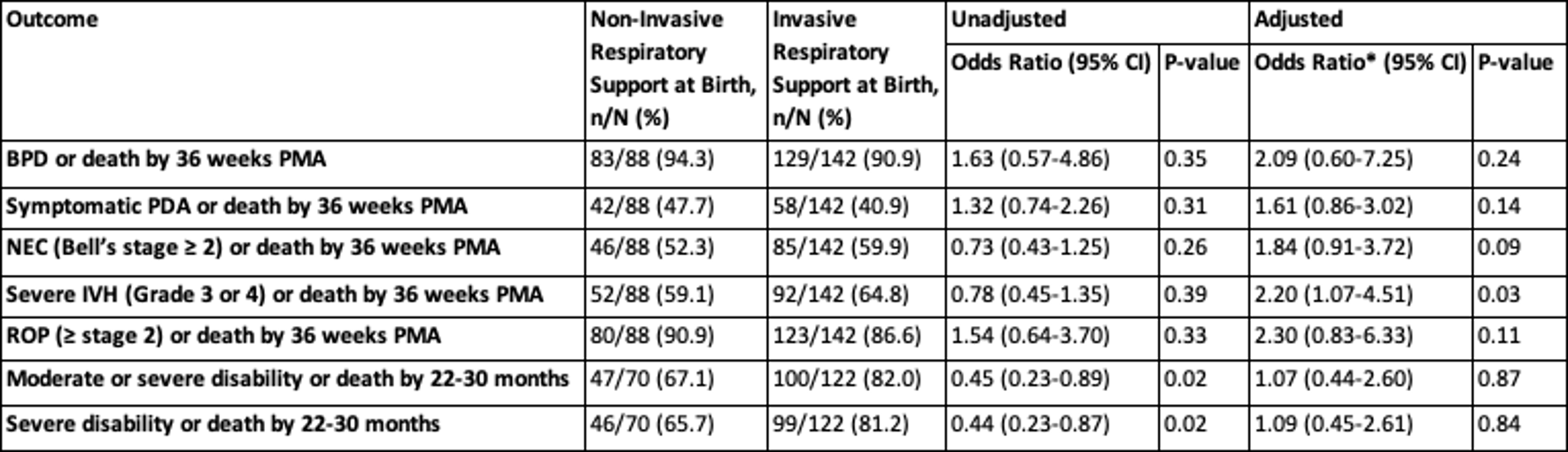 *Adjusted for antenatal corticosteroids, birth weight, gestational age by logistic regression analyses. The adjusted odds ratios represented in the table are for non-Invasive respiratory support at birth group. BPD = bronchopulmonary dysplasia, PMA = post-menstrual age, PDA = patent ductus arteriosus, NEC = necrotizing enterocolitis, IVH = intraventricular hemorrhage, ROP = retinopathy of prematurity.
*Adjusted for antenatal corticosteroids, birth weight, gestational age by logistic regression analyses. The adjusted odds ratios represented in the table are for non-Invasive respiratory support at birth group. BPD = bronchopulmonary dysplasia, PMA = post-menstrual age, PDA = patent ductus arteriosus, NEC = necrotizing enterocolitis, IVH = intraventricular hemorrhage, ROP = retinopathy of prematurity.