
Nephrology: Clinical
Category: Abstract Submission
Nephrology III: General Nephrology and Dialysis

Cal H. Robinson, MD
Pediatric Nephrology Fellow
The Hospital for Sick Children
Toronto, Ontario, Canada
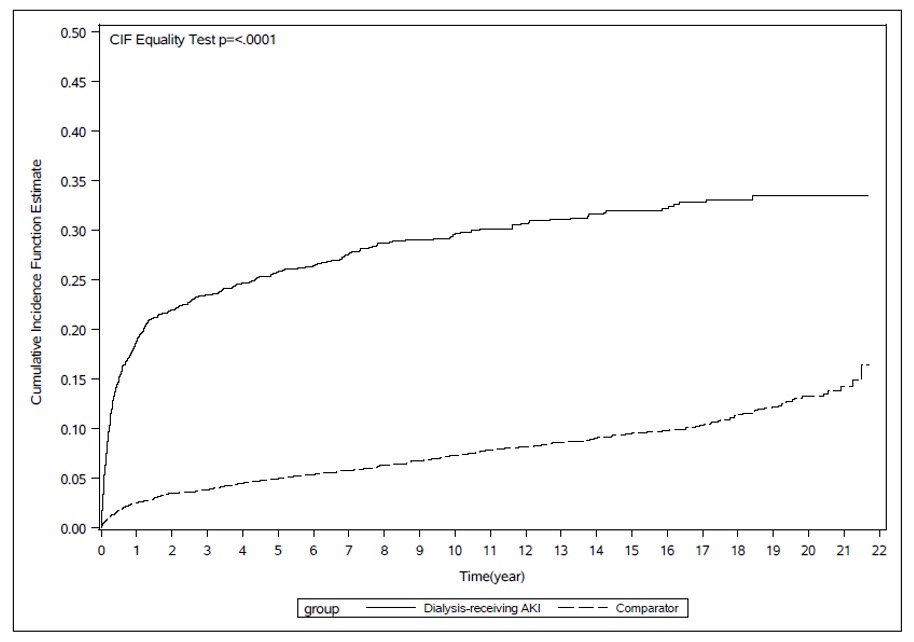 The index date was defined as 104 days post-index hospitalization discharge date. Dialysis-treated AKI survivors experienced nephrologist visits significantly sooner than hospitalized comparators. The greatest difference was observed within the first year after the index date. By 20 years post-hospitalization, only one-third of dialysis-treated AKI survivors had seen a nephrologist.
The index date was defined as 104 days post-index hospitalization discharge date. Dialysis-treated AKI survivors experienced nephrologist visits significantly sooner than hospitalized comparators. The greatest difference was observed within the first year after the index date. By 20 years post-hospitalization, only one-third of dialysis-treated AKI survivors had seen a nephrologist. *p-value < 0.05
*p-value < 0.05