
Infectious Diseases
Category: Abstract Submission
Infectious Diseases: Potpourri

Evin S. Feldman, MD
Resident
NewYork-Presbyterian Morgan Stanley Children's Hospital
Long Island City, New York, United States
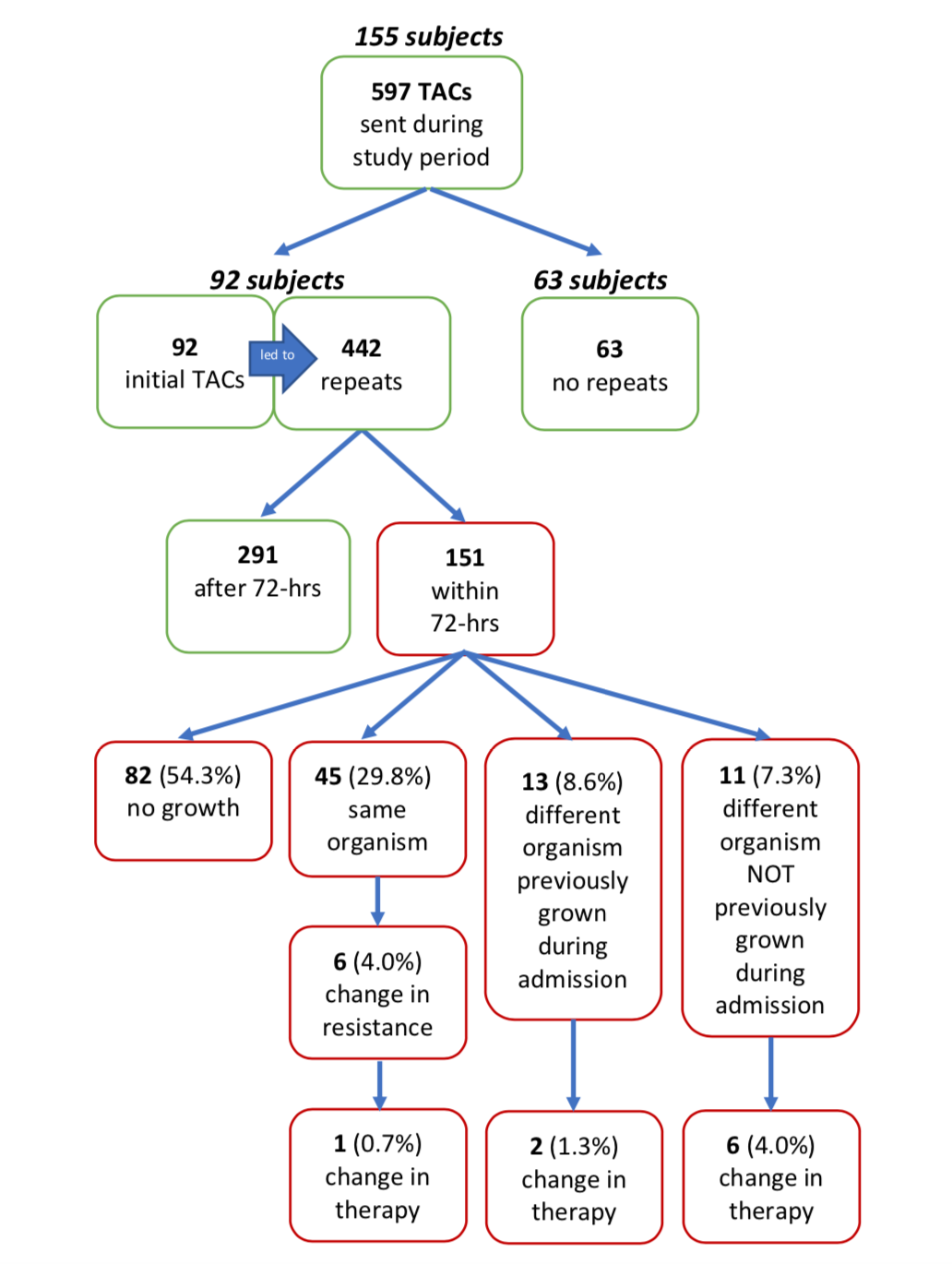 Diagnostic outcomes of tracheal aspirate cultures (TACs). Percentages based off 151 TACs repeated within 72-hours.
Diagnostic outcomes of tracheal aspirate cultures (TACs). Percentages based off 151 TACs repeated within 72-hours.