
Nephrology: Clinical
Category: Abstract Submission
Nephrology III: General Nephrology and Dialysis

Christian Hanna, MD, MS
Assistant professor of Pediatrics
Mayo Clinic Children's Center
Mayo Clinic Minnesota
Rochester, Minnesota, United States
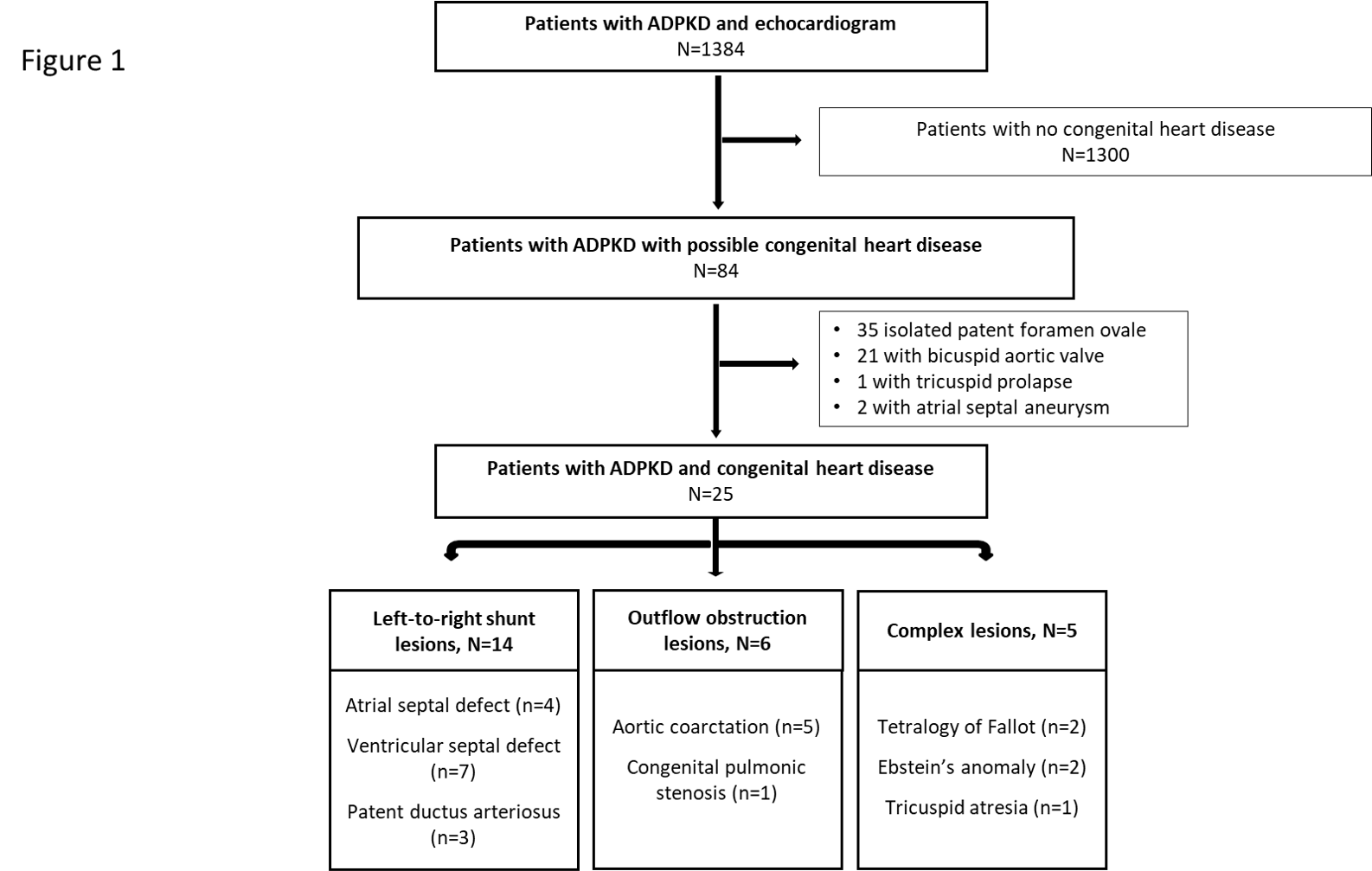 Overview of study flow chart and cohort selection depicting patient exclusions and group assignment based on congenital heart disease subgroups. ADPKD, autosomal dominant polycystic kidney disease; PFO, patent foramen ovale; BAV, bicuspid aortic valve; ASD, atrial septal defect; VSD, Ventricular septal defect; PDA, patent ductus arteriosus.
Overview of study flow chart and cohort selection depicting patient exclusions and group assignment based on congenital heart disease subgroups. ADPKD, autosomal dominant polycystic kidney disease; PFO, patent foramen ovale; BAV, bicuspid aortic valve; ASD, atrial septal defect; VSD, Ventricular septal defect; PDA, patent ductus arteriosus.