
Emergency Medicine: All Areas
Category: Abstract Submission
Emergency Medicine VIII
Joyce Li, MD MPH (she/her/hers)
Assistant Professor in Pediatrics and Emergency Medicine
Boston Children's Hospital
Medford, Massachusetts, United States
.jpg) a American Indian, Asian, Native Hawaiian, multiracial, other race/ethnicity
a American Indian, Asian, Native Hawaiian, multiracial, other race/ethnicity 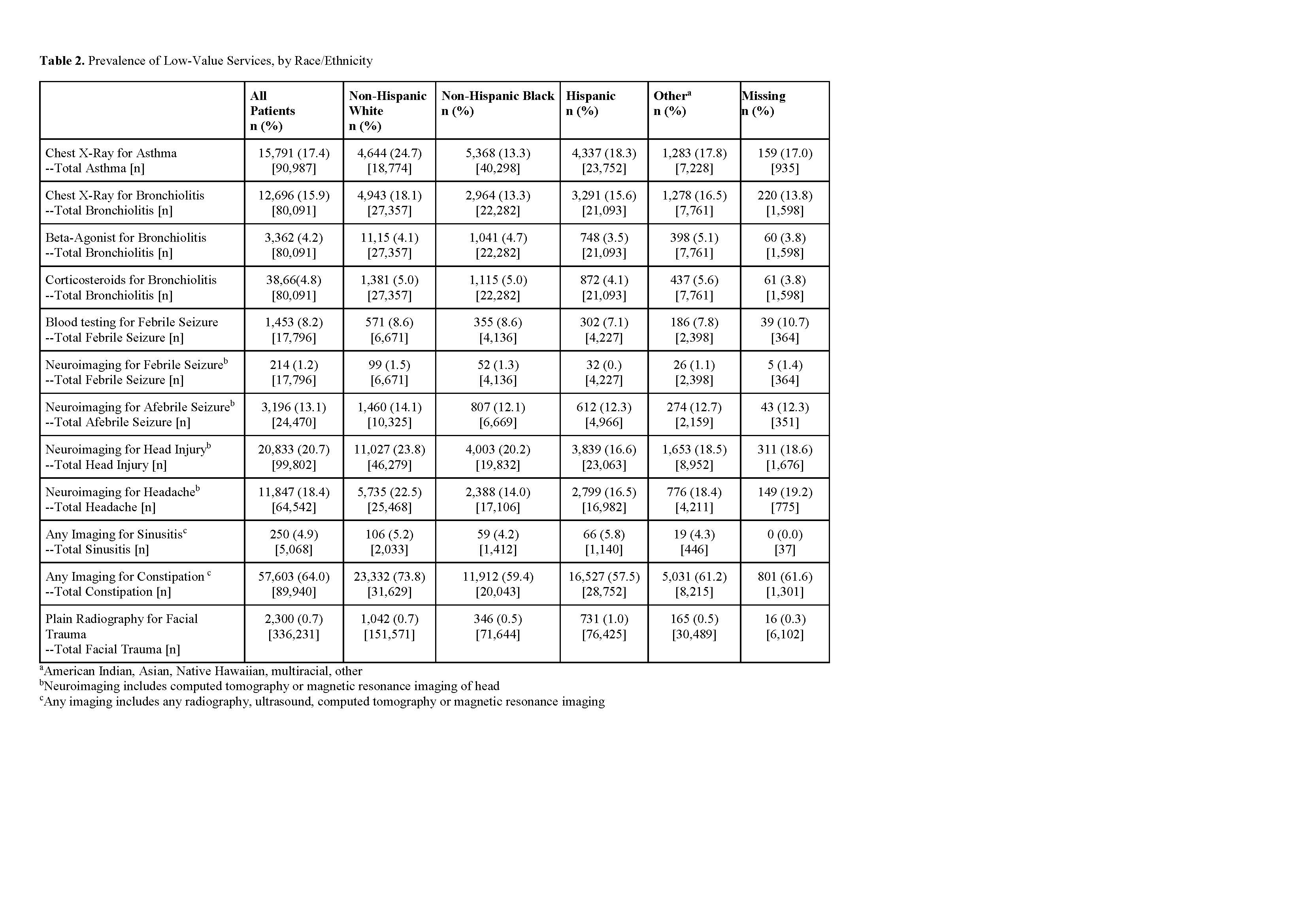 a American Indian, Asian, Native Hawaiian, multiracial, other
a American Indian, Asian, Native Hawaiian, multiracial, other