
Neonatal Pulmonology
Category: Abstract Submission
Neonatal Pulmonology V: Preclinical studies and Clinical Care Issues

Anup Katheria, MD
Physician
Sharp Mary Birch Hospital for Women & Newborns
San Diego, California, United States
.jpg)
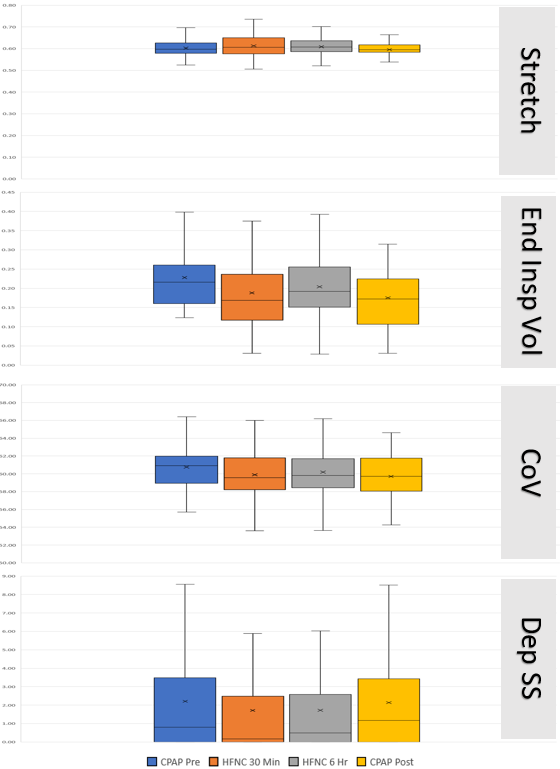 Figure 1 Box and Whisker plot over each period (Stretch, CoV, Center of Ventilation; Dep SS, dependent silent spaces as a percentage of lung;, Volume, end insp vol, end-inspiratory lung volume). CPAP Pre- CPAP at the start of the study, HFNC 30min- 30 minutes of High-flow Cannula, HFNC 6hrs- 6 hours of High-flow cannula, CPAP post- 1 hour after return to CPAP. X denotes mean value otherwise median and 25th and 75th percentiles are shown.
Figure 1 Box and Whisker plot over each period (Stretch, CoV, Center of Ventilation; Dep SS, dependent silent spaces as a percentage of lung;, Volume, end insp vol, end-inspiratory lung volume). CPAP Pre- CPAP at the start of the study, HFNC 30min- 30 minutes of High-flow Cannula, HFNC 6hrs- 6 hours of High-flow cannula, CPAP post- 1 hour after return to CPAP. X denotes mean value otherwise median and 25th and 75th percentiles are shown.