491 - Karenia Brevis red tide toxin exposure and congenital biliary atresia: is there an association?
Monday, April 25, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 491 Publication Number: 491.424
Rita Wyrebek, Johns Hopkins All Children's Hospital, St. Petersburg, FL, United States; Jamie L. Fierstein, Johns Hopkins All Children's Hospital, St. Petersburg, FL, United States; Rebecca G. Wells, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, United States; Joana S. Machry, Johns Hopkins All Childrens Hospital, Saint Petersburg, FL, United States; Sara Karjoo, University of South Florida, Tampa, FL, United States
Neonatologist Saint Louis University, Cardinal Glennon Children's Hospital St. Louis, Missouri, United States
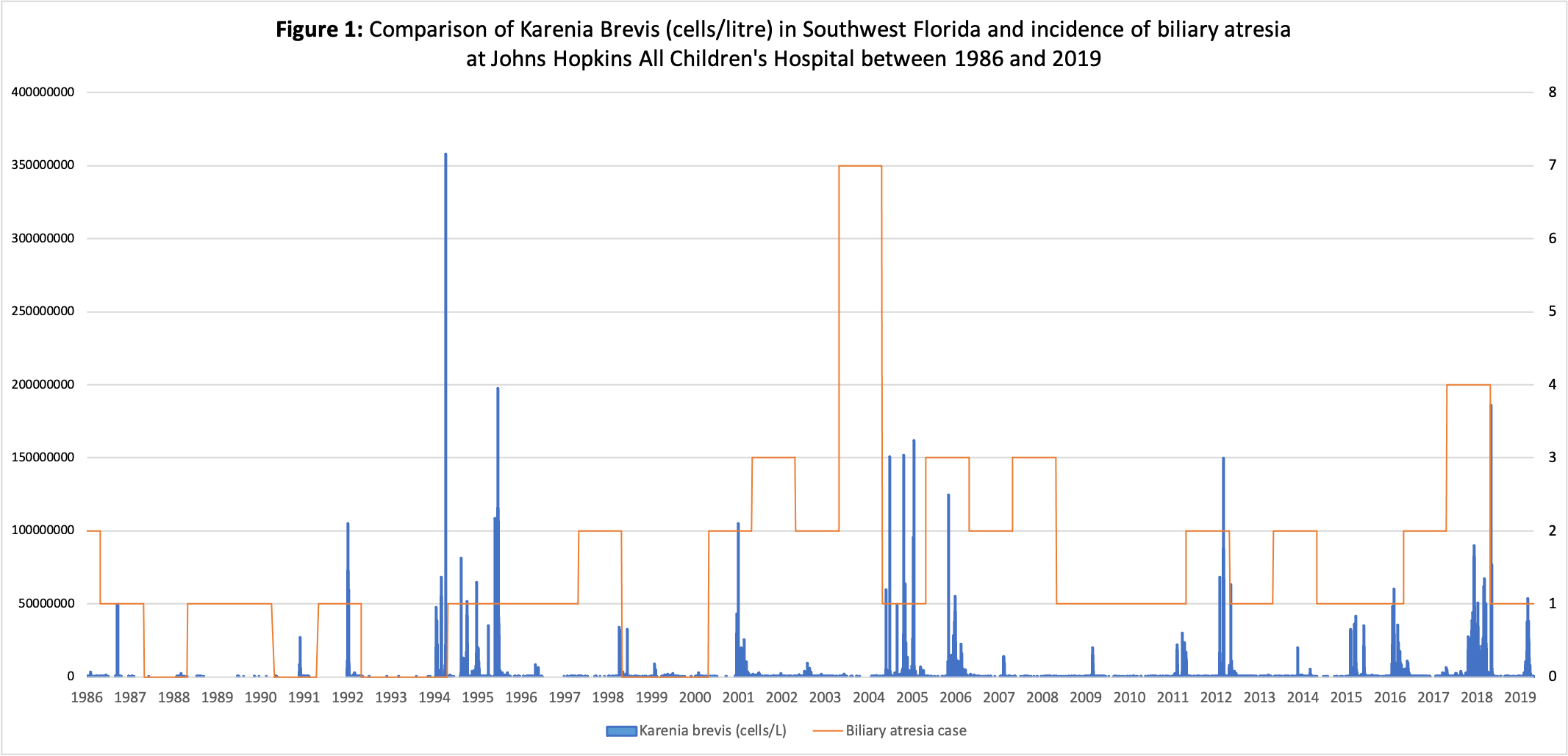
Background: Exposure to environmental toxins (i.e., biliatresone) is a possible mechanism underlying the development of biliary atresia (BA), a progressive fibrocystic liver disease. Brevetoxin (Btx), produced by algae Karenia brevis (KB) and exacerbated by water pollution, has been implicated in causing deleterious developmental effects on marine wildlife; Btx is concentrated in animal livers and excreted in bile. Levels of KB are monitored in Florida and years with the highest reported concentration of KB have coincided with the highest reported incidence of BA (Figure 1).
Objective: Evaluate the association between KB exposure during pregnancy and BA.
Design/Methods: Case control study. Cases (CB): infants diagnosed with BA at Johns Hopkins All Children’s Hospital from January 2000 to December 2019. Controls (CT): random infants, matched 1:4 for birth month, admitted to the hospital during the study period. We excluded patients with congenital anomalies and non-Florida residents. KB (cells/liter) levels at 10- and 50-mile radii were assessed per month of gestation by the Florida Wildlife Commission. We compared variables between groups using Mann-Whitney U tests or Fisher’s Exact tests. Conditional logistic regression showed odds of BA based on maximum KB exposure per trimester for 10- and 50- mile radii adjusted for coastal residence. Two-sided p-values < .05 were considered statistically significant.
Results: There were 38 CB and 152 CT of which 47.4% and 58.6% were coastal residents (p = 0.2). Majority of CT resided in Pinellas County (53%) while CB were from Hillsborough (26%), Pinellas (26%), or Pasco (11%) counties. Among CB, the median of the monthly average gestational exposure at 10-miles was 0 (IQR: 0-888.9) and among CT the median was 222.16 (IQR:0-286,740.7; p=.02). Table 1 shows the maximum exposure per trimester of pregnancy and at 10- or 50-mile radius. Table 2a and 2b show the distribution of maximum exposure per trimester of pregnancy by exposure category. Through matched analyses, higher exposure during all trimesters at 10-miles was associated with lower odds for BA (AOR < 1.0, p≥.5 for all). However, higher exposure during second and third trimesters at 50-miles was associated with increased odds for BA (2nd AOR: 3.4 [95% CI:0.6-20.4], p=0.2; 3rd AOR: 1.7 [95%CI: 0.3-11.4], p=0.6). None of the adjusted analyses reached statistical significance.Conclusion(s): We did not observe a statistically significant association between KB exposure in pregnancy and BA, although other environmental factors or toxins may contribute to the multifactorial pathophysiology of this complex disease. Comparison of Karenia Brevis (cells/litre) in Southwest Florida and incidence of biliary atresia at Johns Hopkins All Children's Hospital between 1986 and 2019 Table 1: Maximum Exposure per Trimester of Pregnancy

 photo")