
Neonatal Quality Improvement
Category: Abstract Submission
Neonatal Quality Improvement IV: Respiratory and Temperature Regulation
 photo")
Daley Owens, MD (she/her/hers)
Resident Physician
Eastern Virginia Medical School
Norfolk, Virginia, United States
.jpg) The corresponding AUC for this model was calculated as 0.772, 95% CI (0.674, 0.871). Moreover, the model had sensitivity/specificity of 34%/97%, 47%/90%, and 66%/76% for cutoff of 60%, 70%, and 80% probability of extubation success, respectively.
The corresponding AUC for this model was calculated as 0.772, 95% CI (0.674, 0.871). Moreover, the model had sensitivity/specificity of 34%/97%, 47%/90%, and 66%/76% for cutoff of 60%, 70%, and 80% probability of extubation success, respectively.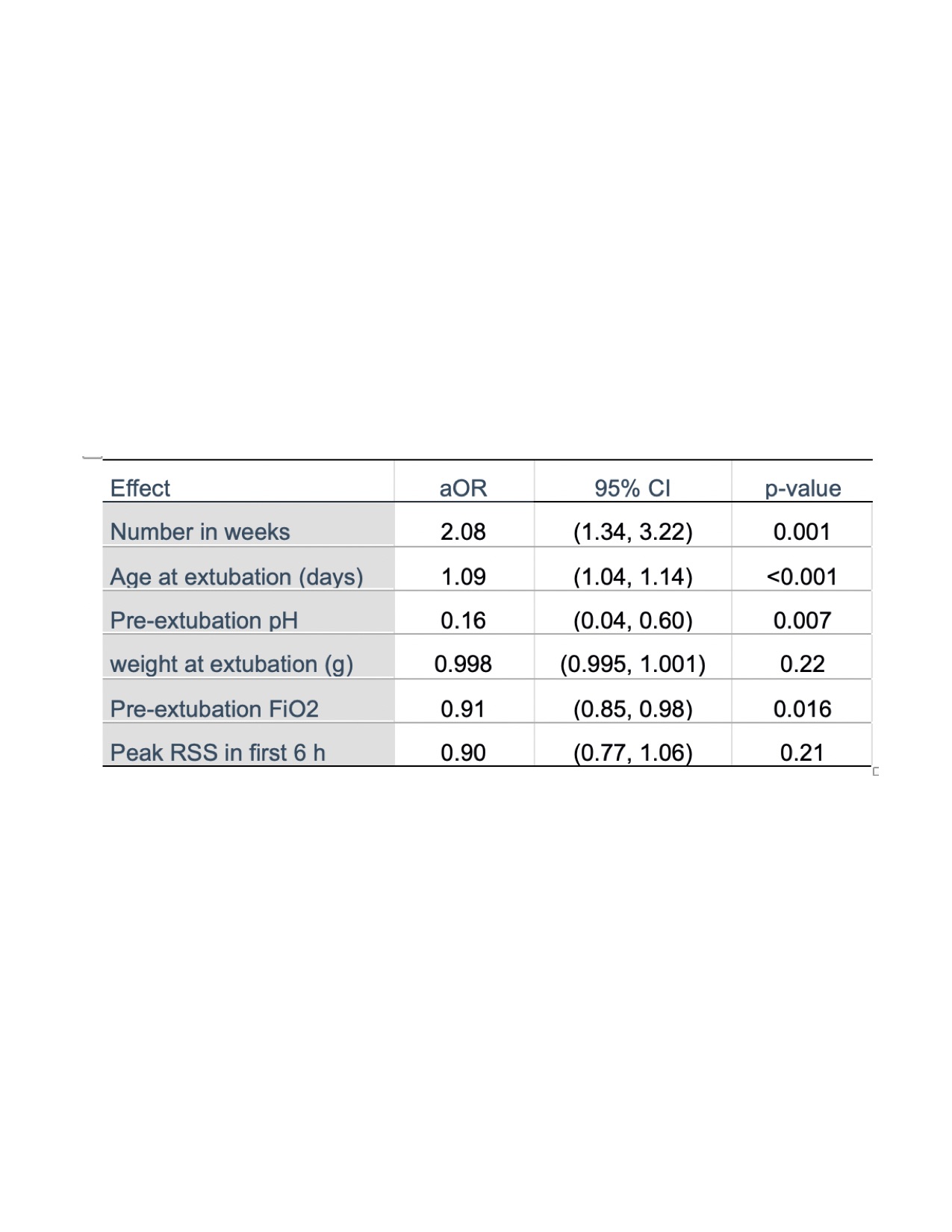 There was a significant association between remaining extubated more than 96 hours and number in weeks (p=0.001), age at extubation (p < 0.001), pre-extubation pH (p=0.007), and pre-extubation FiO2 (p=0.016),
There was a significant association between remaining extubated more than 96 hours and number in weeks (p=0.001), age at extubation (p < 0.001), pre-extubation pH (p=0.007), and pre-extubation FiO2 (p=0.016),