
Neonatal Infectious Diseases/Immunology
Category: Abstract Submission
Neonatal Infectious Diseases/Immunology: Sepsis

David Van Laere, MD
Neonatal Intensive Care Specialist
University Hospital Antwerp
Edegem, Antwerpen, Belgium
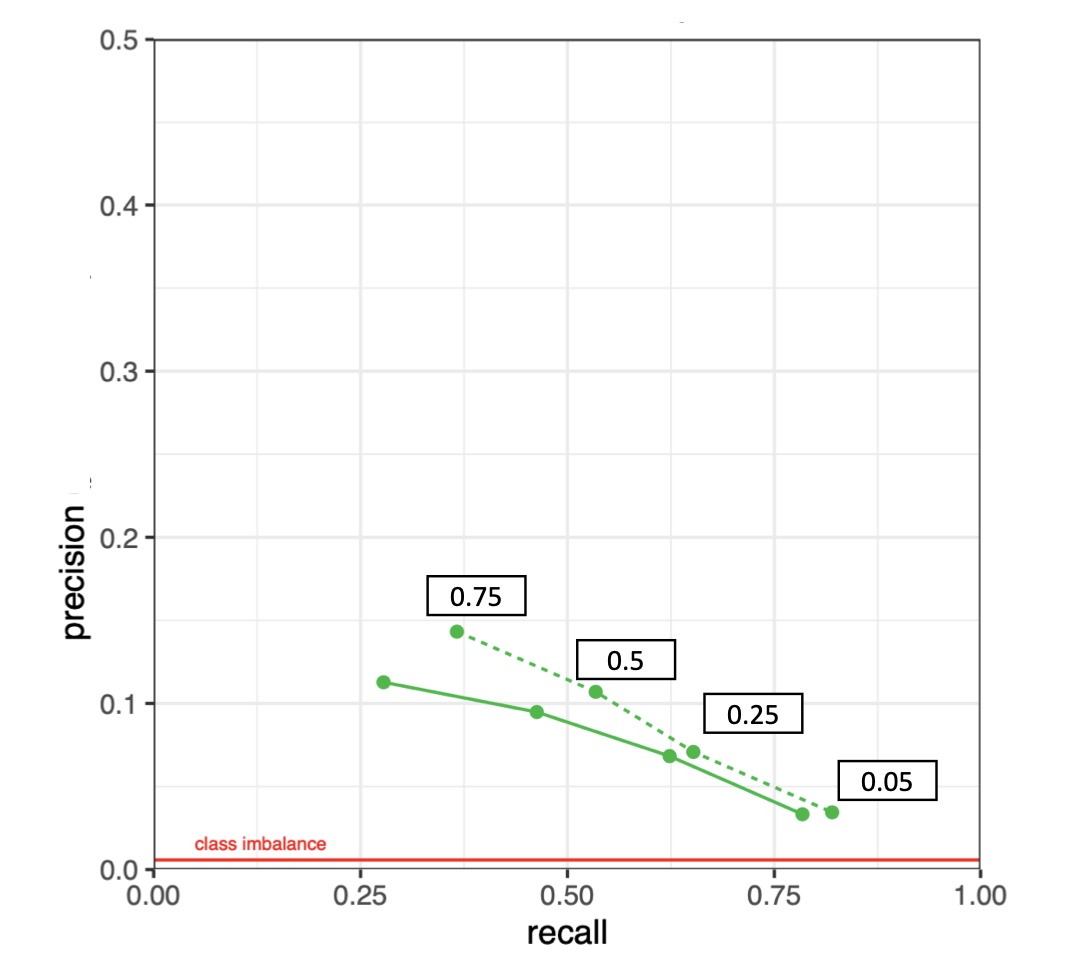 Figure 1: Precision-recall curve showing the performance of the ML model on the retrospective dataset (n=953): The amount of detected sepsis episodes are visualized on the x-axis, together with the model’s precision (y-axis) for the 4 different model probability output thresholds (black boxes).
Figure 1: Precision-recall curve showing the performance of the ML model on the retrospective dataset (n=953): The amount of detected sepsis episodes are visualized on the x-axis, together with the model’s precision (y-axis) for the 4 different model probability output thresholds (black boxes).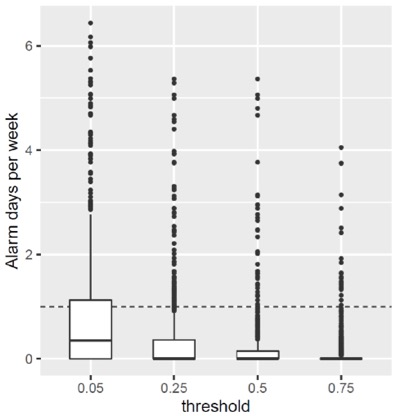 Figure 2: Boxplot representing median and interquartile range of the number of alarm days per week (y-axis) above a certain prediction threshold (x-axis) for patients in the retrospective dataset (n=953). An alarm day is defined as an increased probability output in a 24 hour time-period. The dashed line represents the threshold of 1 patient- alarm per week.
Figure 2: Boxplot representing median and interquartile range of the number of alarm days per week (y-axis) above a certain prediction threshold (x-axis) for patients in the retrospective dataset (n=953). An alarm day is defined as an increased probability output in a 24 hour time-period. The dashed line represents the threshold of 1 patient- alarm per week.