523 - Follow up of presumed NAFLD in community health: QI efforts in a large safety net institution
Saturday, April 23, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 523 Publication Number: 523.239
Kathy Love-Osborne, University of Colorado School of Medicine, Denver, CO, United States; Carina Kugelmas, Denver Health Meedical Center, Denver, CO, United States; Melissa Wong, University of Colorado, Denver, CO, United States; Jeanelle Sheeder, University of Colorado School of Medicine, Aurora, CO, United States
Associate professor University of Colorado School of Medicine Denver, Colorado, United States
Background: Non-alcoholic fatty liver disease (NAFLD) is the most common reason that patients are referred for liver transplant in adults. The AAP recommends screening obese youth for NAFLD with alanine aminotransferase (ALT). Our previous protocol recommended further evaluation of youth with persistent ALT > 100 U/l, but previous cohorts showed 26% of youth had no follow-up testing. NASPGHAN guidelines recommend further evaluation of youth with ALT > 80 U/l for more than 6 months, or ALT > 150 U/l.
Objective: 1. Increase % of youth with elevated ALT that have follow-up testing. 2. Increase % of youth with evaluation for alternate etiologies of elevated liver enzymes if indicated
Design/Methods: Participants: youth with 1st time ALT elevation ≥80 U/L Setting: community health network caring for medically underserved youth in Denver, CO Electronic chart review was performed and youth with other primary diagnoses or symptoms were excluded. Demographics, previous, 1st >80 U/L, next and last ALT, date and BMI at time of ALT, and results of further testing was collected. Upper limit of normal for sex was defined as 22 U/l for girls and 26 for boys. 3 cohorts were developed with initial ALT elevation (U/l) of: #1: >100 between 1/14 and 3/16 (n=140) #2: >100 between 7/16 and 5/18 (n=172) #3: >80 between 5/18 and 9/19 (n=165) In fall of 2018, primary care providers (PCPs) at this institution were educated to schedule follow up of index ALT ≥80 U/L in 1 month for a hepatic panel, assessment for etiologies other than NAFLD, and lifestyle referral if the family agreed. Further evaluation was recommended for youth with ALT >150 U/l at follow-up or persistent ALT elevation >80 U/l at 6 months. Providers were instructed to add elevated ALT to the problem list if it was ≥30 U/l.
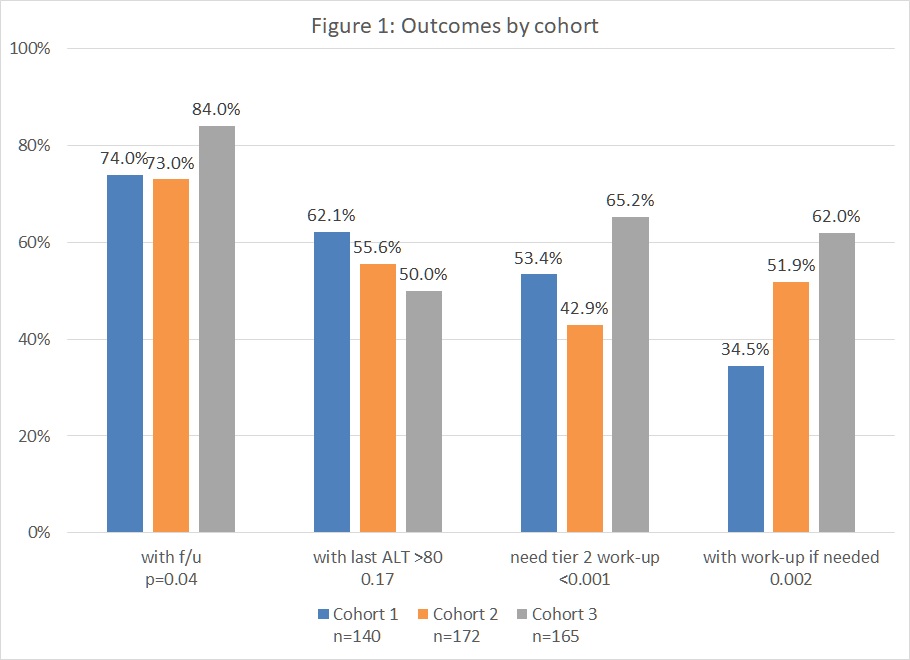
Results: Demographics were similar in all cohorts, with mean age 13.3 years, BMI 31.5, 78% male and 91% Hispanic. 162 youth had previous ALT measurement. Only 4% were below the ULN for gender on previous ALT. Figure 1 describes outcomes of youth with follow up and evaluation for etiologies other than NAFLD.Conclusion(s): Implementation of a shared care model involving PCP follow up of youth with presumed NAFLD improved follow-up rates and appropriate evaluation for alternate etiologies of elevated liver enzymes. The finding that 96% of youth presenting with an initial ALT >80 U/L had previously abnormal ALT illustrates the importance of identifying probable NAFLD earlier and addressing the diagnosis with families. PCP involvement is critical to decrease the future need for liver transplant in this high-risk population. Figure 1: outcomes by cohort