21 - Cardiac Recovery in Children Admitted to the Pediatric Intensive Care Unit with Multisystem Inflammatory Syndrome in Children
Friday, April 22, 2022
6:15 PM – 8:45 PM US MT
Poster Number: 21 Publication Number: 21.102
Zelda Ghersin, Hackensack Meridian Health, Neptune City, NJ, United States; Andrew Corson, K. Hovnanian Children's Hospital at Jersey Shore University Medical Center, Neptune, NJ, United States; Sara Galeotti, K. Hovnanian Children's Hospital at Jersey Shore University Medical Center, Ocean, NJ, United States; Stephanie Chin, K. Hovnanian Children's Hospital at Jersey Shore University Medical Center, Brick, NJ, United States; Hannah Kim, Joseph M. Sanzari Children's Hospital Hackensack University Medical Center, Hackensack, NJ, United States; saranga Agarwal, Pediatric intensive care , Hackensack University Medical Center, Hackensack, NJ, United States
Pediatric Resident K. Hovnanian Children's Hospital at Jersey Shore University Medical Center Neptune, New Jersey, United States
Background: Multi-System Inflammatory Syndrome in Children (MIS-C) is a post-acute infection dysregulated inflammatory response that occurs four to six weeks after SARS-CoV-2 infection. Up to 80% of patients hospitalized with MIS-C develop cardiac complications. Due to low incidence of disease and limited data, there is no clear consensus on predictors of cardiac recovery or the cardiac outcomes in patients with MIS-C.
Objective: To evaluate the short and midterm cardiac outcomes in children hospitalized with MIS-C in two pediatric intensive care units (PICU) in New Jersey.
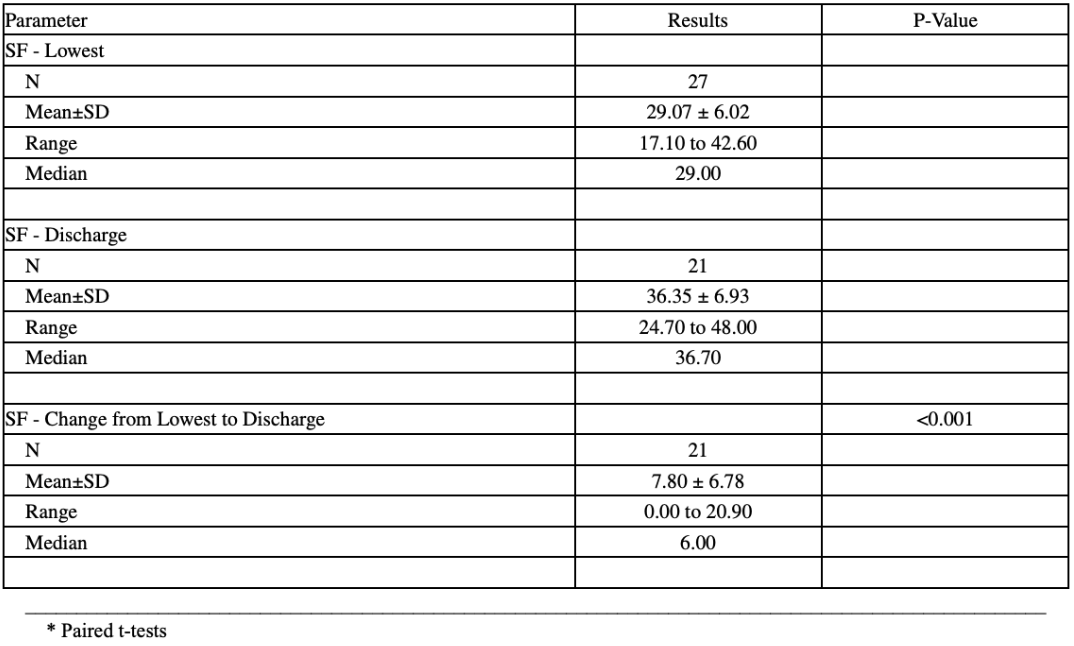
Design/Methods: We conducted a retrospective review of children admitted to the PICU with a diagnosis of MIS-C between April 2020 through March 2021. Cardiac biomarkers and echocardiograms performed during hospitalization were analyzed. Follow-up echocardiograms were performed two to eight weeks post-discharge, with interval follow-up of up to one year. Shortening fraction (SF) was used to assess left ventricular systolic function using standard M-mode (SF < 28% considered abnormal).
Results: Twenty-seven patients (18 male; median age 11 years) were included. The mean peak Troponin I in 25 patients was 2.10 +/- 5.0 ng/dL, and mean peak NT-ProBNP level in 26 patients was 1,606 +/- 1293 pg/dL. Most patients had normalization of cardiac biomarkers by time of discharge (Table 1). Seven of the 23 patients who had an echocardiogram on admission had a SF less than 28%. Lowest SF and SF at the time of discharge were compared in 21 patients with a median improvement of 6% (p < 0.001) (Table 2). Nineteen patients had a follow-up echocardiogram two to ten weeks post discharge and 18 of those had normal left ventricular systolic function (p < 0.001). No patient had evidence of diastolic dysfunction at follow-up. Eight patients had midterm follow-up five to seven months post-discharge, and one patient was followed for one-year post-discharge. Abnormalities that persist in these patients include low normal left ventricular systolic function. Three subjects had evidence of left coronary artery dilation (z score >2) during hospitalization and continued to have diffuse dilation at follow-up; with one developing right coronary artery dilation.Conclusion(s): In this cohort of patients, most children admitted to the PICU with MIS-C had abnormal cardiac biomarkers with normal to mildly decreased left ventricular systolic function that improved by time of discharge and continued to improve with midterm (5-7 months) follow-up. A very small subset of patients, however, continue to have cardiac complications including diffuse coronary artery dilation. Table 1


.png)