
Critical Care
Category: Abstract Submission
Critical Care I
Grace E. Logan, MD
Pediatric Critical Care Fellow
Children's Hospital Colorado
Denver, Colorado, United States
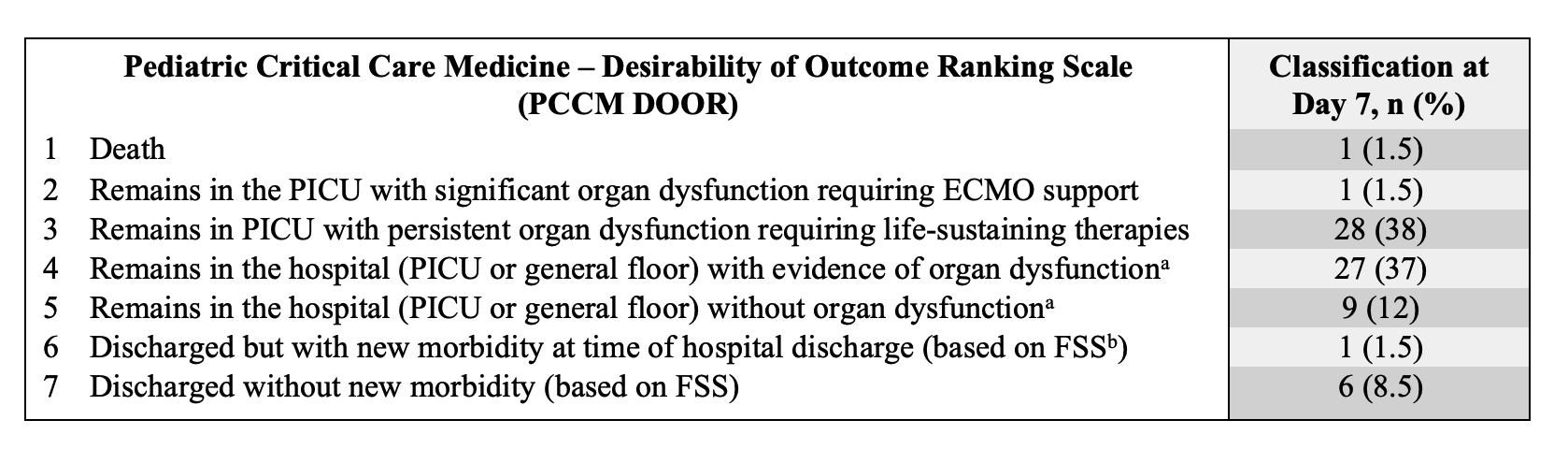 The scale was modified from the World Health Organization (WHO) Clinical Progression Scale, which is currently being used to assess outcomes in interventional trials in patients with respiratory failure due to SARS-CoV-2 infection.
The scale was modified from the World Health Organization (WHO) Clinical Progression Scale, which is currently being used to assess outcomes in interventional trials in patients with respiratory failure due to SARS-CoV-2 infection.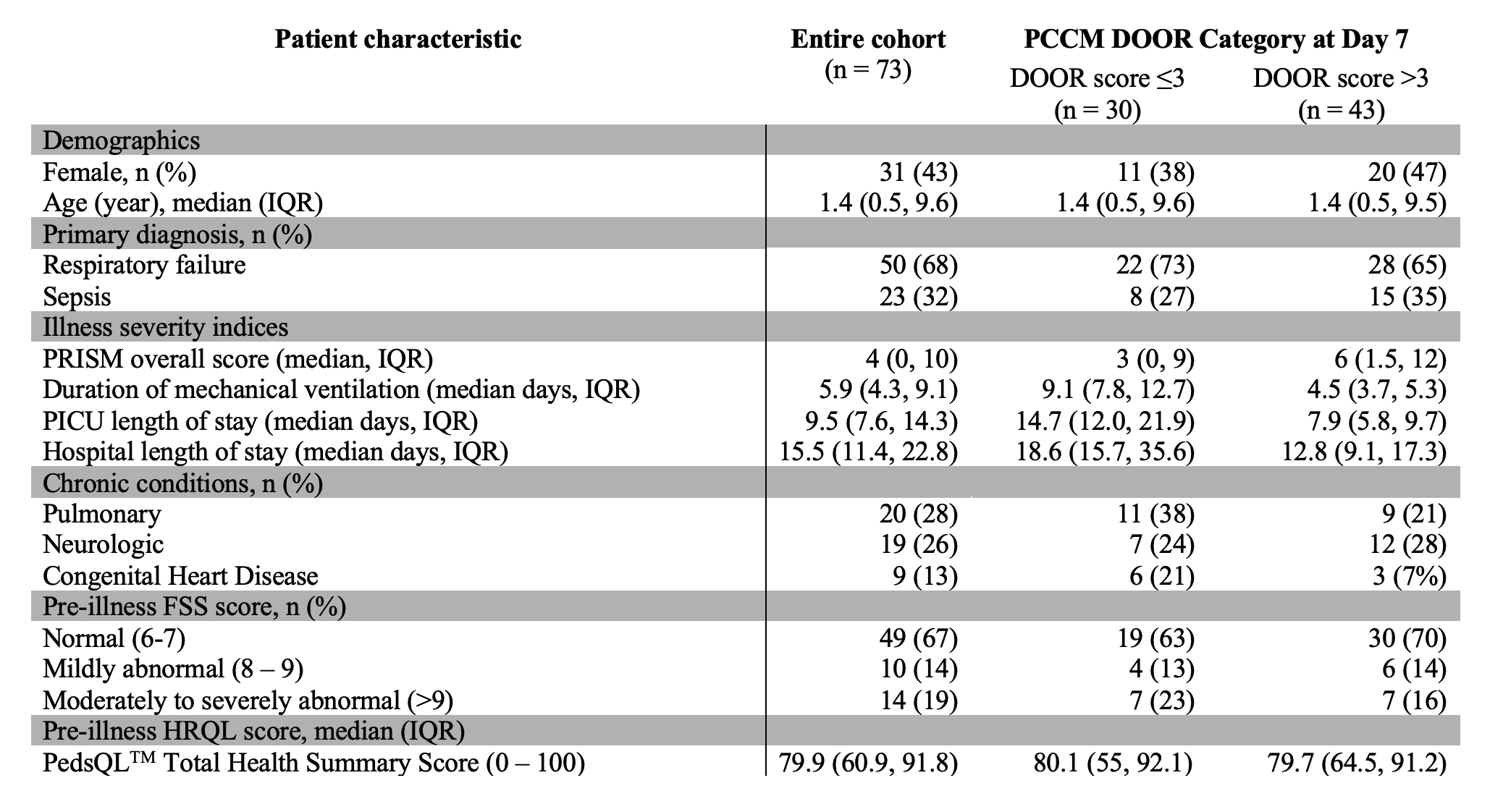 PICU: Pediatric Intensive Care Unit; PRISM: Pediatric Risk of Mortality Score; PCCM DOOR: Pediatric Critical Care Medicine Desirability of Outcome Ranking; IQR: Interquartile Range; FSS: Functional Status Scale
PICU: Pediatric Intensive Care Unit; PRISM: Pediatric Risk of Mortality Score; PCCM DOOR: Pediatric Critical Care Medicine Desirability of Outcome Ranking; IQR: Interquartile Range; FSS: Functional Status Scale