
Hospital Medicine: Clinical
Category: Abstract Submission
Hospital Medicine: Clinical - Bronchiolitis/HFNC and Newborn Care

Kimiko S. Dunbar, MD
Pediatric Hospital Medicine Fellow
Children's Hospital Colorado
Denver, Colorado, United States
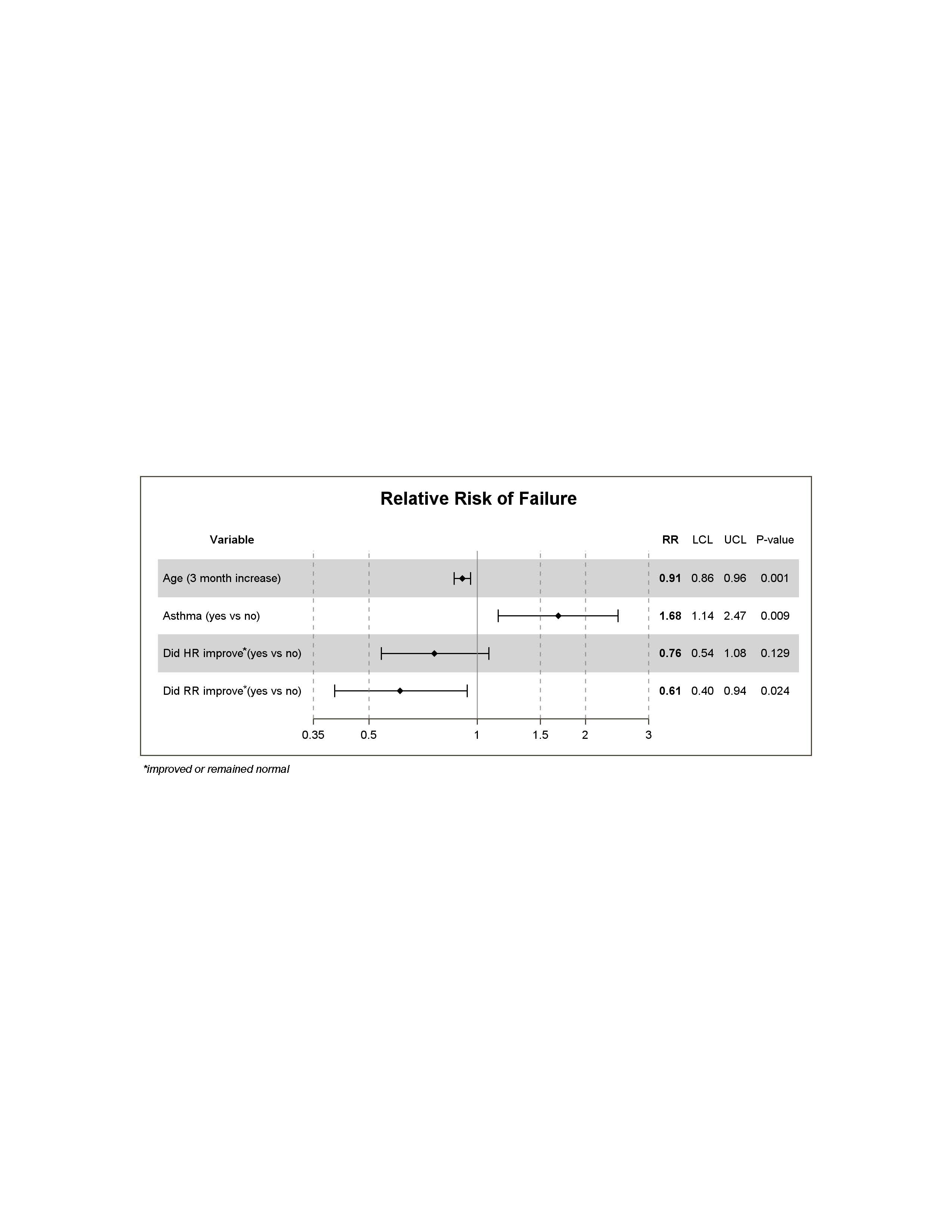 Relative Risk of Failure
Relative Risk of Failure