
Neonatal General
Category: Abstract Submission
Neonatology General 11: Lung
 photo")
David Healy, MB, BaO, Bch, BSc (he/him/his)
Research Fellow
University College Cork
Cork, Cork, Ireland
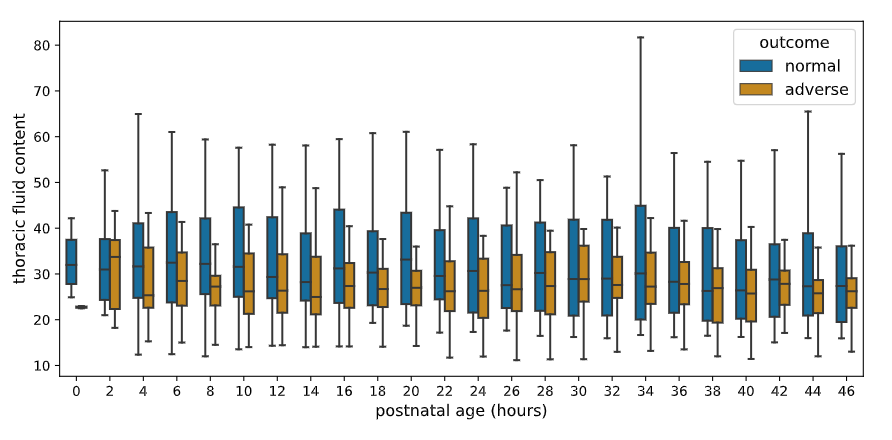 Box plots for median TFC values over 2-hourly windows for the first 48 hours of life and grouped by adverse compared to normal outcome.
Box plots for median TFC values over 2-hourly windows for the first 48 hours of life and grouped by adverse compared to normal outcome.