
Neonatal General
Category: Abstract Submission
Neonatology General 8: Health Disparities - Health Services Research

Nancy Yang, BA
Clinical Research Assistant
Childrens Hospital of Philadelphia
Philadelphia, Pennsylvania, United States
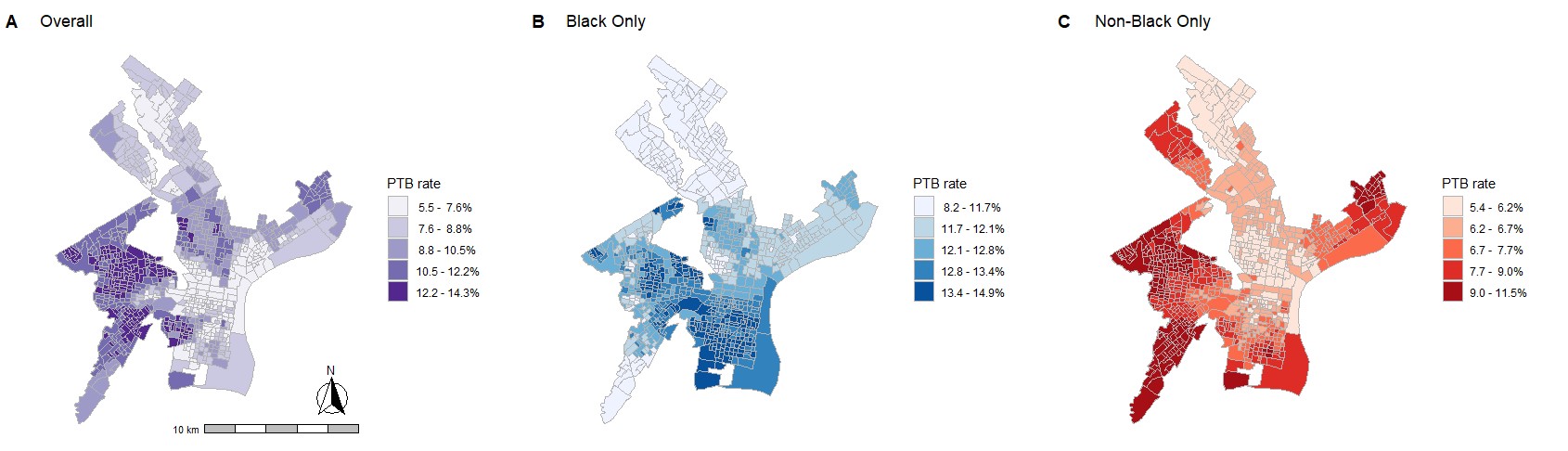 Spatial patterns of PTB rate among the overall population, Black patients, and non-Black patients
Spatial patterns of PTB rate among the overall population, Black patients, and non-Black patients.jpg) Spatial patterns of sPTB and mPTB rates among the overall population, Black patients, and non-Black patients
Spatial patterns of sPTB and mPTB rates among the overall population, Black patients, and non-Black patients