
Hospital Medicine: Clinical
Category: Abstract Submission
Hospital Medicine: Clinical - Infectious Disease NOS

Jillian Cotter, MD, MSCS
Pediatric Hospitalist
University of Colorado / Children's Hospital Colorado
Aurora, Colorado, United States
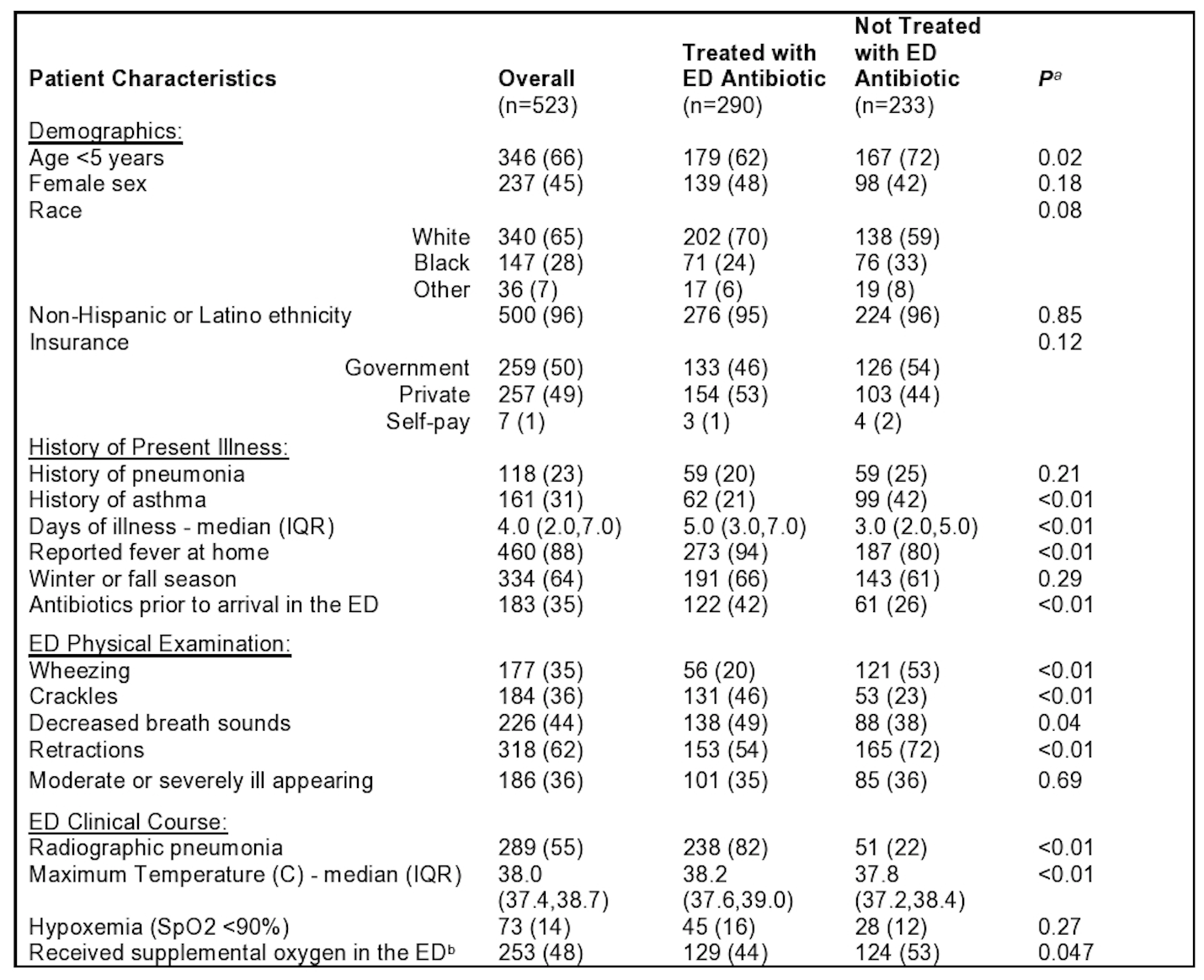 Values represent N(%) unless otherwise specified.
Values represent N(%) unless otherwise specified.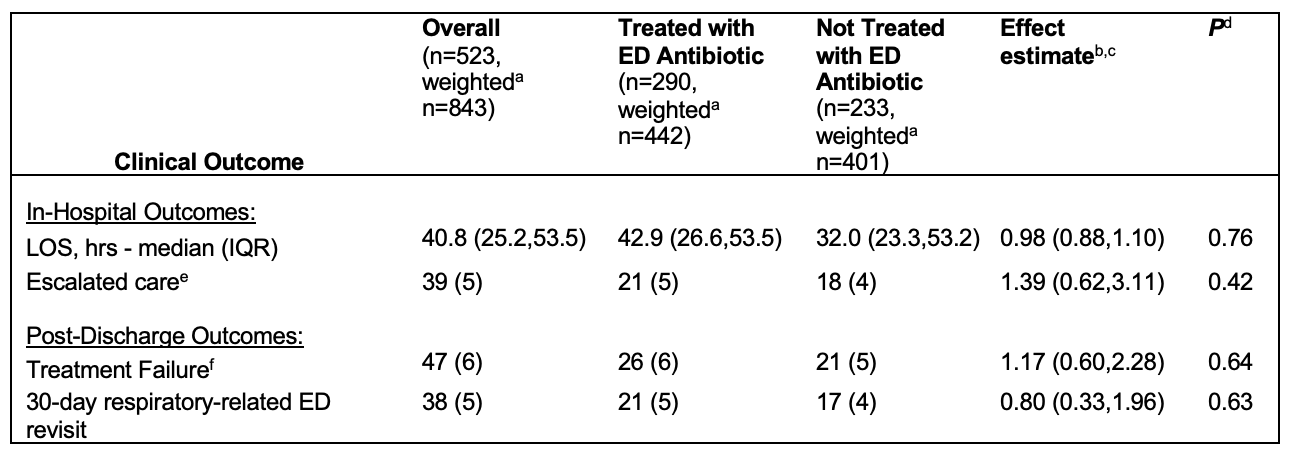 Values represent N(%) from weighted bivariable analysis unless otherwise stated.
Values represent N(%) from weighted bivariable analysis unless otherwise stated.