
Global Neonatal & Children's Health
Category: Abstract Submission
Global Child and Adolescent Health I

Nora Switchenko, MD
Assistant Professor
University of Alabama at Birmingham
Homewood, Alabama, United States
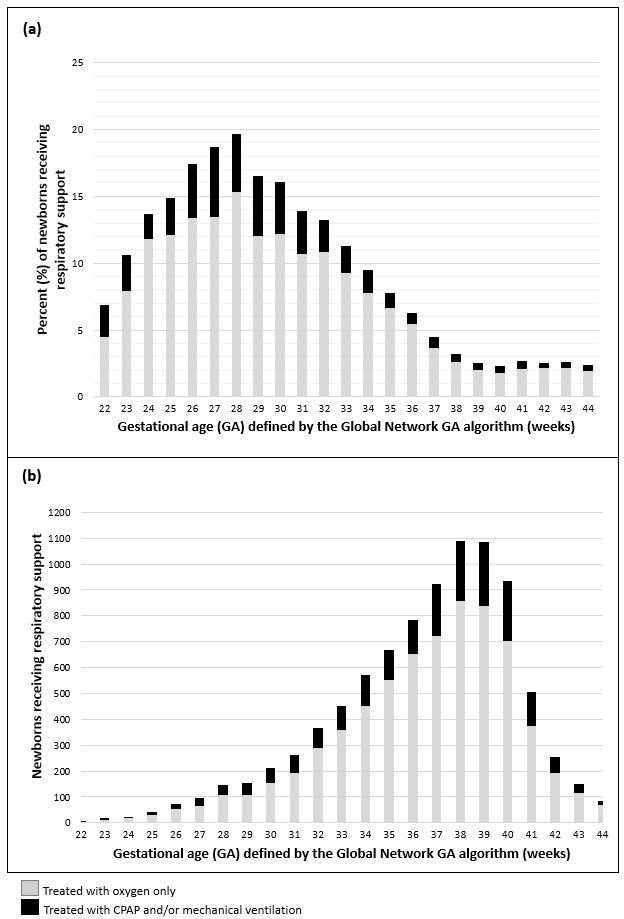 (a) Rate of respiratory support treatment by gestational age defined by the Global Network gestational age algorithm. The proportion of newborns that received respiratory support increased with decreasing gestational age. (b) The number of newborns that received respiratory support by gestational age. The number of newborns that received respiratory support increased with increasing gestational age.
(a) Rate of respiratory support treatment by gestational age defined by the Global Network gestational age algorithm. The proportion of newborns that received respiratory support increased with decreasing gestational age. (b) The number of newborns that received respiratory support by gestational age. The number of newborns that received respiratory support increased with increasing gestational age.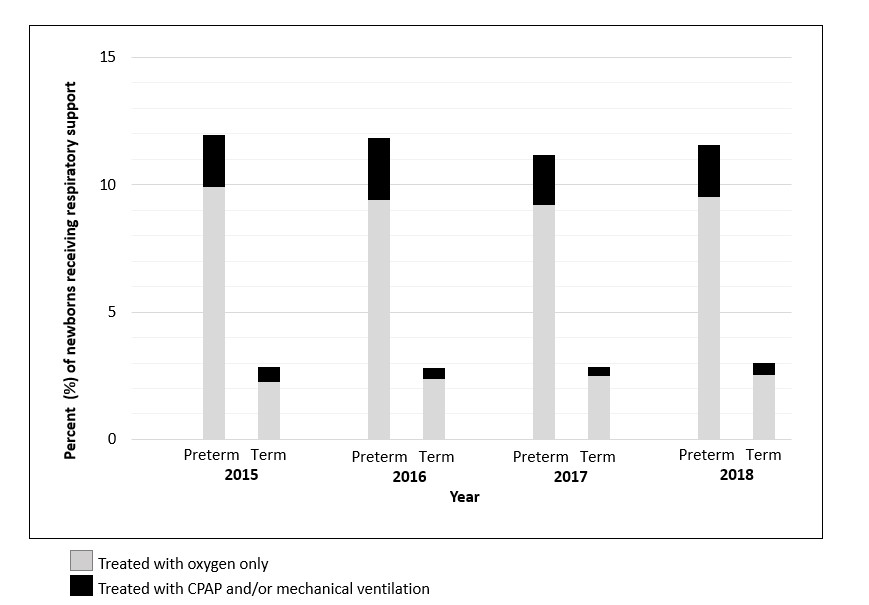 Rate of respiratory support treatment by year. In preterm infants, there was no change in the rate of receipt of respiratory support. In term infants, there was a small increase in the rate of receipt of oxygen only.
Rate of respiratory support treatment by year. In preterm infants, there was no change in the rate of receipt of respiratory support. In term infants, there was a small increase in the rate of receipt of oxygen only.