334 - Association of placental pathology and neonatal hematologic outcomes
Friday, April 22, 2022
6:15 PM – 8:45 PM US MT
Poster Number: 334
Andrew Franklin, Northshore university healthsysten, Evanston, IL, United States; Alexa Freedman, NorthShore University HealthSystem, Evanston, IL, United States; Linda M. Ernst, University of Chicago Division of the Biological Sciences The Pritzker School of Medicine, Evanston, IL, United States
Neonatologist Northshore University Healthsysten Evanston, Illinois, United States
Background: Neonatal hematologic parameters are affected by the in utero environment. However, the role of placental pathologic diseases on the neonate are not well characterized. We hypothesize that abnormal placental pathology, particularly maternal and fetal vascular malperfusion (MVM, FVM), will adversely affect neonatal hematologic outcomes.
Objective: To investigate how neonatal hematologic outcomes (complete blood count (CBC), red cell (RC) and platelet (PLT) transfusions (tx), and need for phototherapy (PT)) vary by major domain of placental histopathology.
Design/Methods: In a single center retrospective cohort of liveborn singleton infants from suburban Chicago between January 2017-June 2021, medical record data was abstracted using Enterprise Data Warehouse. Placental pathology reports were reviewed by a single experienced placental pathologist and subsequently coded into individual placental lesions. Placental pathology was divided into four major domains of placental pathology (acute inflammation (AI), chronic inflammation (CI), MVM, FVM). Levels of severity (none, low, high grade for each domain) were determined based on previously published data; severe grade lesions are described in results. Data were abstracted for infant’s first CBC, PT use, and RC and PLT tx. Analysis was done using multivariable linear regression for continuous variables and binary logistic regression for dichotomous variables adjusted for all other placental pathologies.
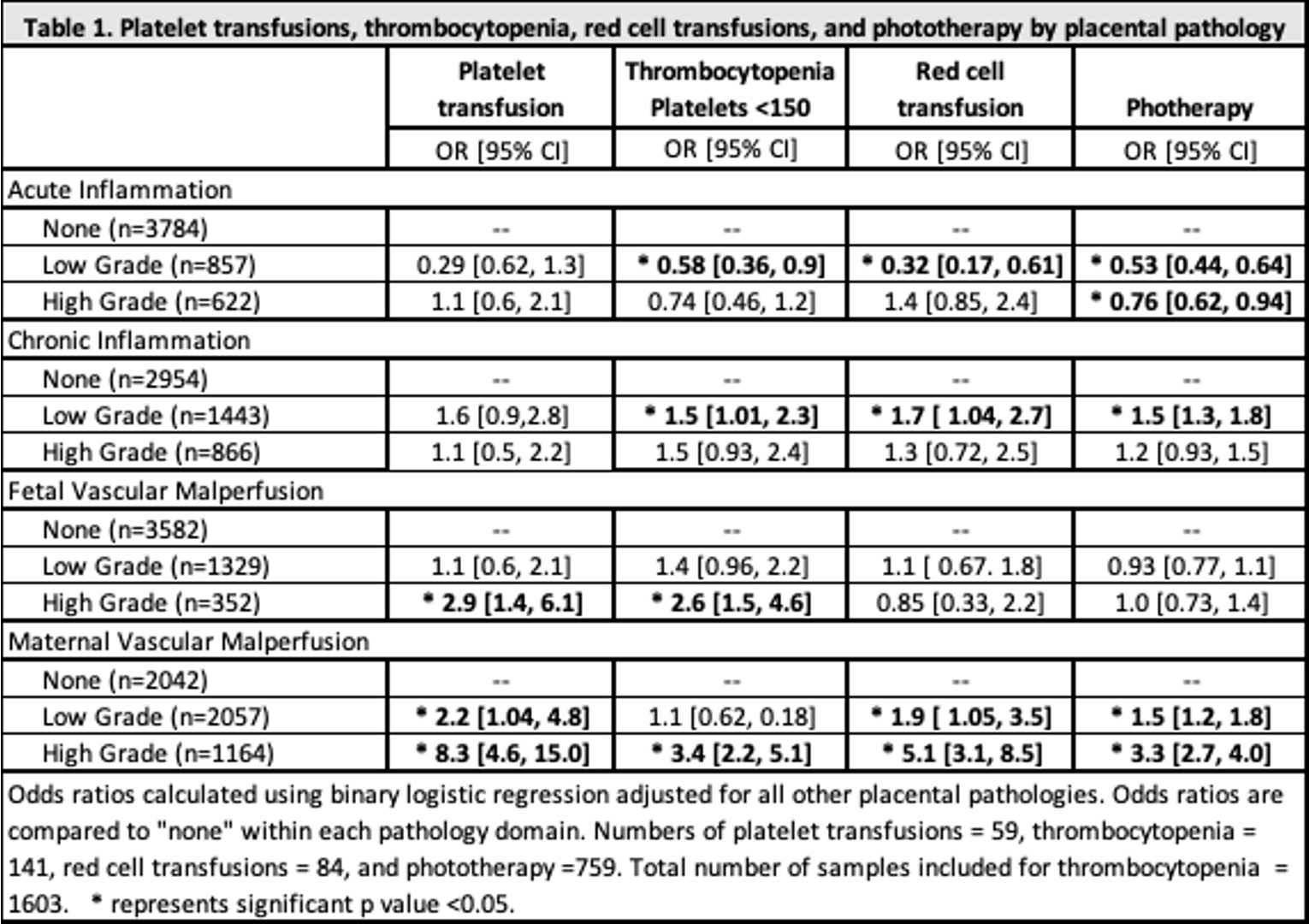
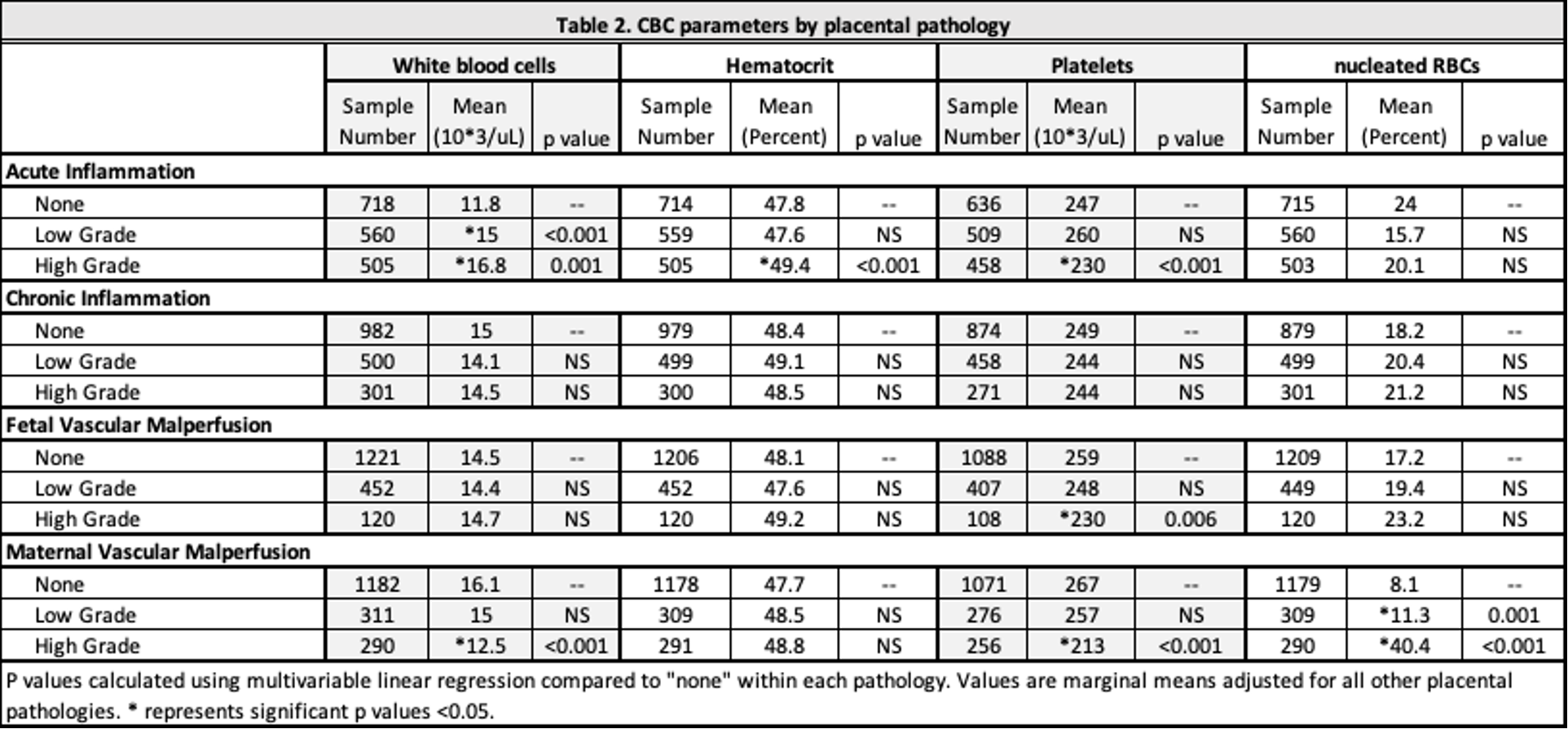
Results: 5263 infants with placental histologic data were including in this study. MVM was associated with increased PT use (OR 3.3 [2.7, 4.0]), RB tx (OR 9.4 [2.2, 40.8]), and PLT tx (OR 8.3 [4.6, 15.0]). PLT tx was increased with FVM (OR 2.9 [1.4, 6.1]). Need for PT was decreased with AI (OR 0.8 [0.6, 0.9]). Of those with available CBC data (n=1603), PLT counts were lower with MVM (213 vs 266, p < 0.001), AI (230 vs 247, p < 0.001), and FVM (230 vs 259, p=0.003). Thrombocytopenia (PLT < 150) was associated with MVM (OR 3.7 [2.2, 5.1]) and FVM (OR 2.6 [1.5, 4.6]). Nucleated RCs were increased with MVM compared to those without MVM (40% vs 8%, p < 0.001). White blood cells were decreased with MVM (12.5 vs 16.1) and higher with AI (16.8 vs 11.8).Conclusion(s): This study shows placental pathology impacts neonatal hematologic outcomes. Infants exposed to MVM have neutropenia, thrombocytopenia, increased need for PT and increased RC and PLT tx compared to those without MVM. Severe MVM predisposes infants for hematologic abnormalities. Further investigation into these mechanisms is warranted. Table 1. Platelet transfusions, thrombocytopenia, red cell transfusions, and phototherapy by placental pathology Table 2. CBC parameters by placental pathology