
Infectious Diseases
Category: Abstract Submission
Infectious Diseases: Bacteria & Antimicrobials
Amanda Nedved, MD
Pediatric Urgent Care Physician
Children's Mercy
UMKC School of Medicine | KU School of Medicine
Lenexa, Kansas, United States
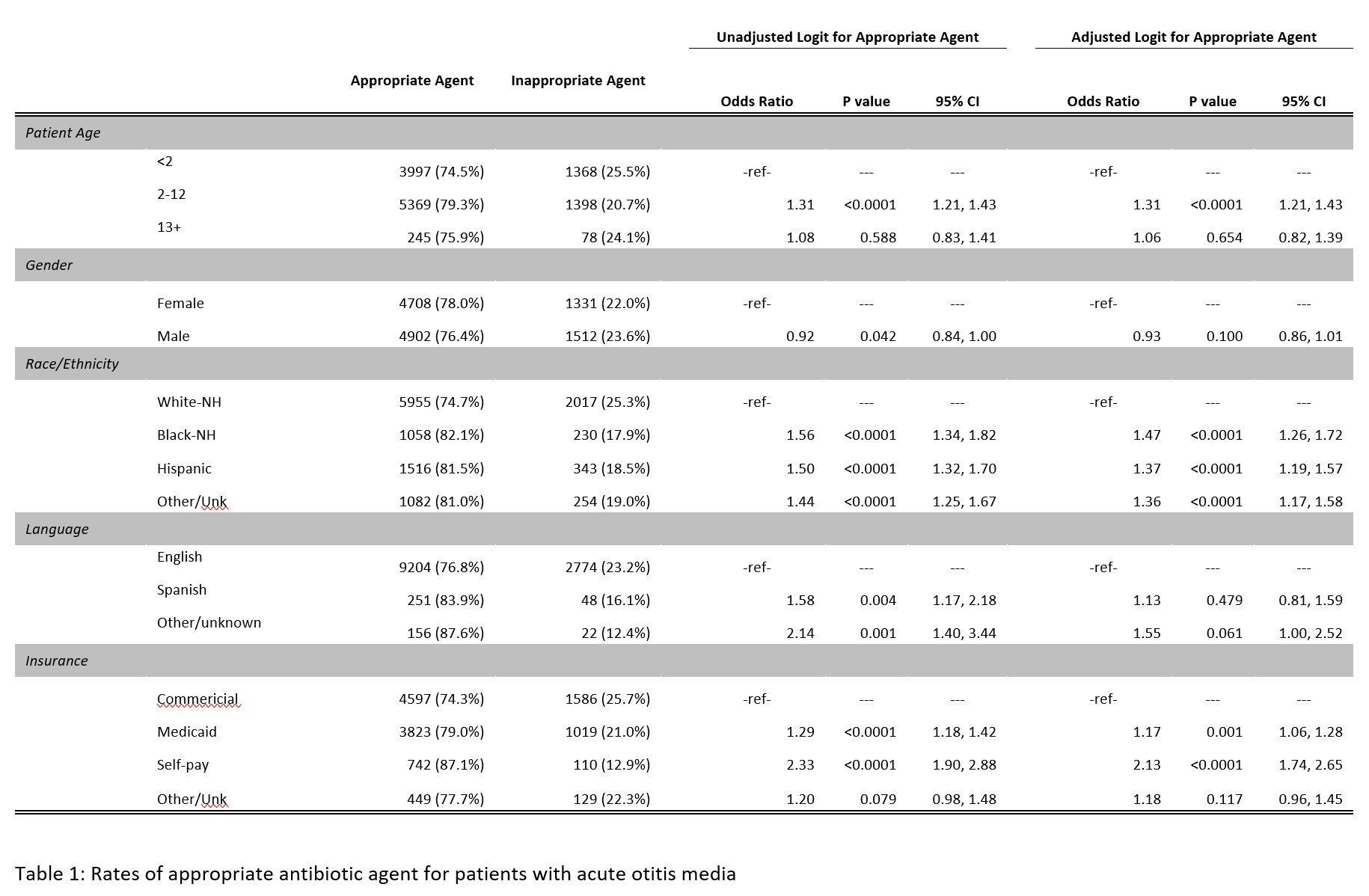 Rates of appropriate antibiotic agent for acute otitis media
Rates of appropriate antibiotic agent for acute otitis media