
Nephrology: CKD
Category: Abstract Submission
Nephrology I: Potpourri
Tarak Srivastava, MD
Attending Nephrologist
Children's Mercy Hospital
Children's Mercy Hospitals and Clinics
Kansas City, Missouri, United States
.png) Median values and interquartile range (parantheses) for the demographic data and the measured urinary eicosanoids in control and children with SK are shown. Generalized Wilcoxon test was used to compare the two groups.
Median values and interquartile range (parantheses) for the demographic data and the measured urinary eicosanoids in control and children with SK are shown. Generalized Wilcoxon test was used to compare the two groups.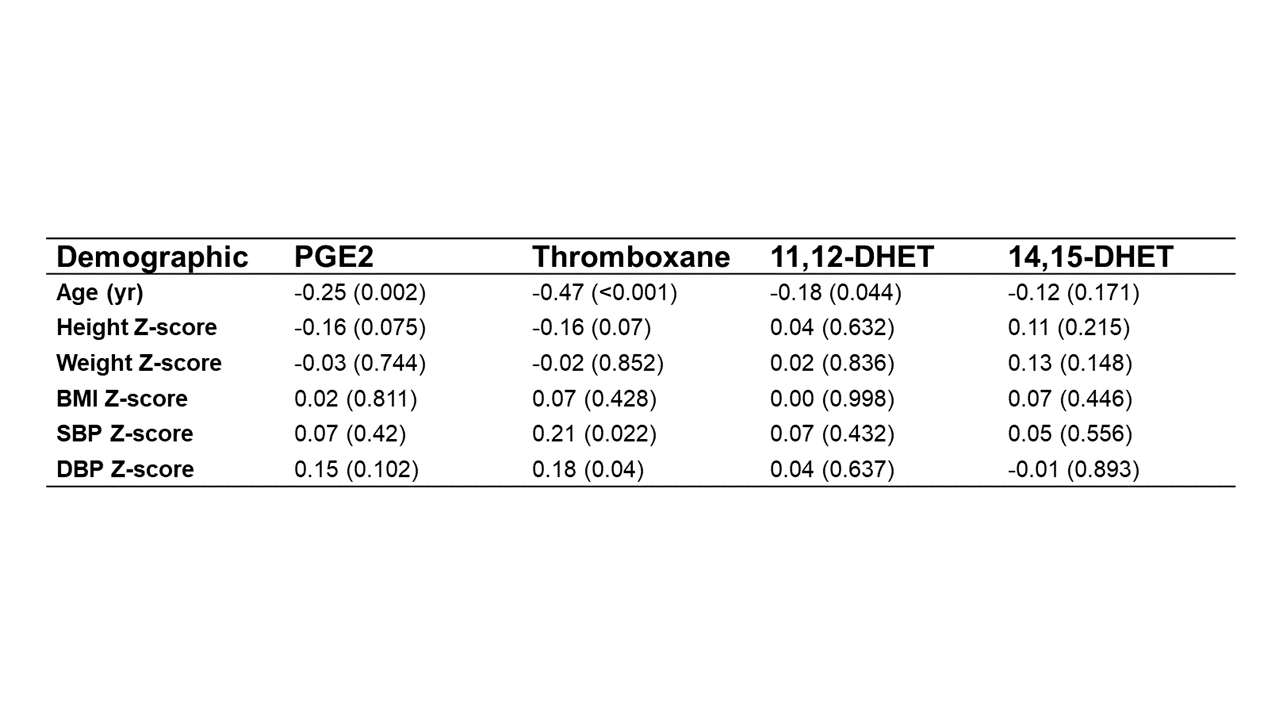 The correlation between PGE2, Thromboxane, 11,12-DHET or 14,15-DHET with the demographic data is shown. Spearman’s correlation analysis was used.
The correlation between PGE2, Thromboxane, 11,12-DHET or 14,15-DHET with the demographic data is shown. Spearman’s correlation analysis was used.