29 - Access to Pediatric Living Donor Kidney Transplants: The Impact of Social Determinants of Health
Saturday, April 23, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 29 Publication Number: 29.235
Eliza Blanchette, Children's Hospital Colorado, Denver, CO, United States; Elizabeth S. Christofferson, University of Colorado School of Medicine, Aurora, CO, United States; SHREY PUROHIT, N/A, Anschutz, CO, United States; Eric G. Benz, Children's Hospital Colorado, Aurora, CO, United States; Kristen McKinnon, Children's Hospital Colorado, Aurora, CO, United States; Megan Bisek, Children's Hospital Colorado, Aurora, CO, United States; Jon Armendariz, Children's Hospital Colorado, Aurora, CO, United States; Margret Bock, University of Colorado School of Medicine, Aurora, CO, United States
Assistant Professor Children's Hospital Colorado Denver, Colorado, United States
Background: Living Donor (LD) kidney transplants (KT) have superior long-term outcomes. In adults’ certain social determinants of health (SDH) and racial/ethnic backgrounds are associated with decreased access to LD KT.
Objective: We aimed to investigate the association between these factors, including the impact of education by a dedicated Spanish-speaking transplant nephrologist for Spanish-speaking patients, in pediatric KT recipients (pKTR) and any resultant impacts on access to LD KT.
Design/Methods: This retrospective cohort study investigated pKTR transplanted between 1/2016-3/2021 at our institution. Data collected included baseline demographics and patient or care giver (CG) report of mental health concerns, substance use, and trauma identified during KT candidate evaluation. Education by a dedicated Spanish-speaking transplant nephrologist for Spanish-speaking patients, during the evaluation process, was tracked. Descriptive statistics were utilized as well as two-sample t-tests, chi square, and logistic regression for tests of significance.
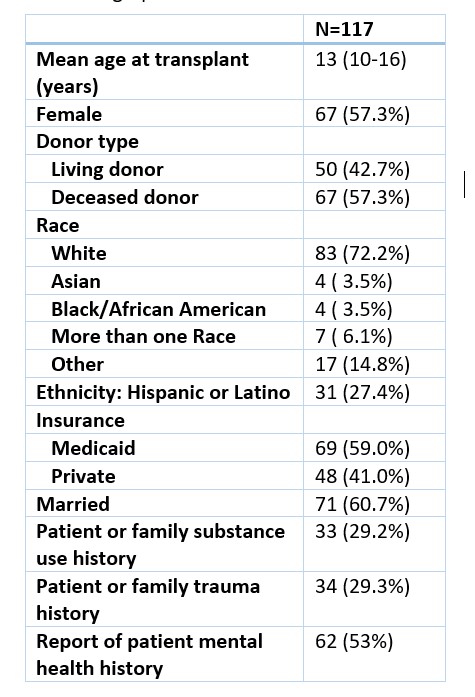
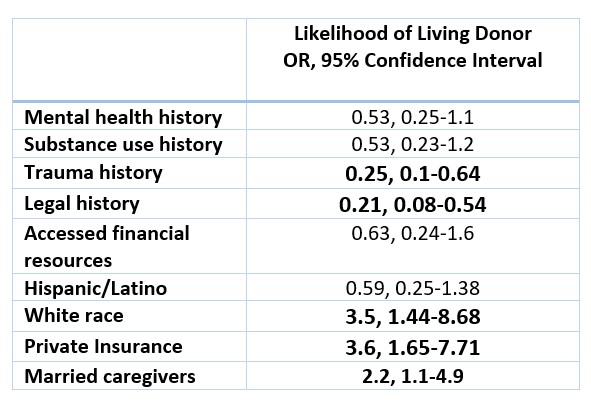
Results: 117 pKTR were included; mean age 13 years (10-16) at time of KT (Table 1). Trauma history and involvement with the legal system were negatively associated with likelihood of receiving a LD KT (OR 0.25, 95% Confidence Interval (CI) 0.1-0.64, OR 0.21, CI 0.08-0.54, respectively). White race (OR 3.5, CI 1.44-8.68), private insurance (OR 3.6, CI 1.65-7.71), and married CG status (OR 2.2, CI 1.1-4.9) were associated with increased likelihood of receiving a LD KT. Hispanic ethnicity was neither associated with increased nor decreased likelihood of LD KT (Table 2). Receipt of education by a Spanish-speaking transplant nephrologist did increase likelihood of receiving a living donor transplant (chi2 4.1, p-value 0.04). In multivariate analysis, only the association of private insurance with increased likelihood of receiving a LD KT maintained statistical significance (OR 2.85, CI 1.05-7.78, Table 3). Conclusion(s): Certain SDH were associated with likelihood of receiving a LD KT in our pediatric cohort. Of note, Hispanic ethnicity was not associated with a decrease likelihood, which is divergent from national adult literature. We hypothesize this may be related to our intervention of education by a Spanish-speaking pKTR and CG with a dedicated Spanish-speaking transplant nephrologist to discuss LD KT. Further interventions and study are needed to help address SDH and LD organ transplant. Table 1: Demographics and Social Determinants of Health Table 2: Associations of Social Determinants of Health and Ethnicity on Receipt of Living Donor Transplant