31 - Clinical Characteristics of Recurrent Focal Segmental Glomerulosclerosis (rFSGS) After Kidney Transplant (KTx) Through Computable Phenotypic Algorithm Analyses of Multi-Center Data
Saturday, April 23, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 31 Publication Number: 31.235
Vikas R. Dharnidharka, Washington University in St. Louis School of Medicine, Creve Coeur, MO, United States; Rebecca R. Scobell, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Mahmoud Kallash, Nationwide Children's Hospital, Columbus, OH, United States; Amy Goodwin Davies, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Nicole Marchesani, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Mitchell Maltenfort, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Leslie Walther, Washington University in St. Louis, St. Louis, MO, United States; Megan Kelton, Seattle Children's, Seattle, WA, United States; Margret Bock, University of Colorado School of Medicine, Aurora, CO, United States; Eliza Blanchette, Children's Hospital Colorado, Denver, CO, United States; Hillarey Stone, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Caroline A. Gluck, NemoursAlfred I. duPont Hospital for Children, Wilmington, DE, United States; Frank Hullekes, Harvard Medical School, Boston, MA, United States; Leonardo Riella, MGH, Boston, MA, United States; William E. Smoyer, Nationwide Children's Hospital, Delaware, OH, United States; Mark Mitsnefes, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Bradley P. Dixon, University of Colorado School of Medicine, Aurora, CO, United States; Joseph Flynn, University of Washington School of Medicine, seattle, WA, United States; Michael Somers, Boston Children's Hospital, Boston, MA, United States; Christopher Forrest, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Susan Furth, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Michelle Denburg, Childrens Hospital of Philadelphia, Philadelphia, PA, United States
Vice-Chair and Nephrology Division Chief Washington University in St Louis Creve Coeur, Missouri, United States
Background: Primary FSGS, a glomerular disease, has a high rate of progression to end stage kidney failure and recurrence after KTx. Reported risk factors for recurrence, efficacy of treatments, and long term outcomes have been difficult to assess given the rarity and heterogeneity of FSGS.
Objective: To determine from multicenter electronic health records (EHR) the characteristics and treatment responses of a contemporary cohort of rFSGS.
Design/Methods: Using the PEDSnet research network of >7 million patients (database v4.0), we applied a published computable phenotype for pediatric glomerular disorders and then selected individuals with a history of nephrotic syndrome who received a KTx between 1/2009 and 11/2020 to form our study sample. Via chart review we identified those KTx patients with FSGS and the subset whose disease recurred (rFSGS; urine protein/creatinine ratio > 2.0 mg/mg post-KTx). Multivariable Cox models used splines to describe time-varying effects of specific treatments, as cumulative doses increased over time.
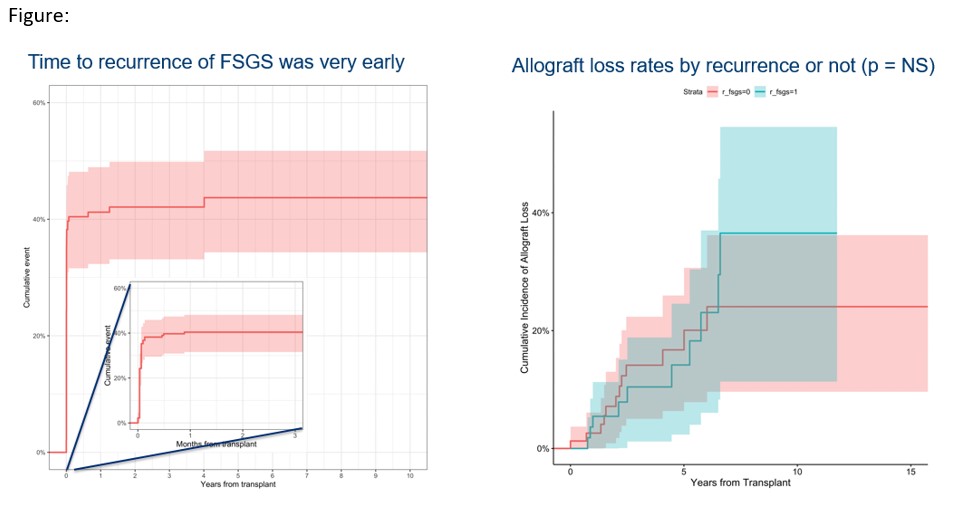
Results: 2294/4968 patients with glomerular disorders were identified as nephrotic. 290 had evidence for KTx. By chart review, 198 had non-genetic FSGS, and 146 received a KTx after 2009. Treatments for rFSGS were identified in 62/146 patients, generally soon after KTx (Fig. Panel A). Demographic characteristics of those with non-recurrent FSGS (n=84) or rFSGS (n=62) are shown in the Table. Plasmapheresis alone (n=18) or with a mAb to CD20 (n=18) were the most common treatments used, followed by lipoprotein-apheresis (n=14), IVIG (n=10) and fusion Ab to CTLA4 (n=6), the last three never in isolation. By 36 months post-transplant, complete remission (CR) occurred in 60% and partial in another 20%. Allograft loss was not significantly worse in those with recurrence (Fig. Panel B). In multivariable models, only mAb to CD20 use was associated with CR (p = 0.0091) and only low density lipoprotein-apheresis (LDL-A) was associated with overall remission (OR; p = 0.048). A greater number of treatments was associated with higher hazard ratios for OR ( >90 plasmapheresis, > 9 LDL-A, > 4 fusion Abs to CTLA4). The hazard ratio of mAb to CD20 with CR was highest with 2-3 doses but dropped to less than one after 5 doses.Conclusion(s): Using EHR data from PEDSnet, we identified rFSGS in 42% of all FSGS patients, most occurring within 3 months of KTx. Age at KTx, sex, or donor source was not associated with recurrence. By 36 months, 80% of patients achieved a CR or OR. Allograft loss was not higher with recurrence. Our data can help inform the design for pragmatic treatment trials for rFSGS. Table Figure


.jpg)