
Nephrology: Transplant
Category: Abstract Submission
Nephrology II: Transplant
Olivia Lullmann, N/A
Undergraduate Research Assistant
University of Iowa Stead Family Children's Hospital
Iowa City, Iowa, United States
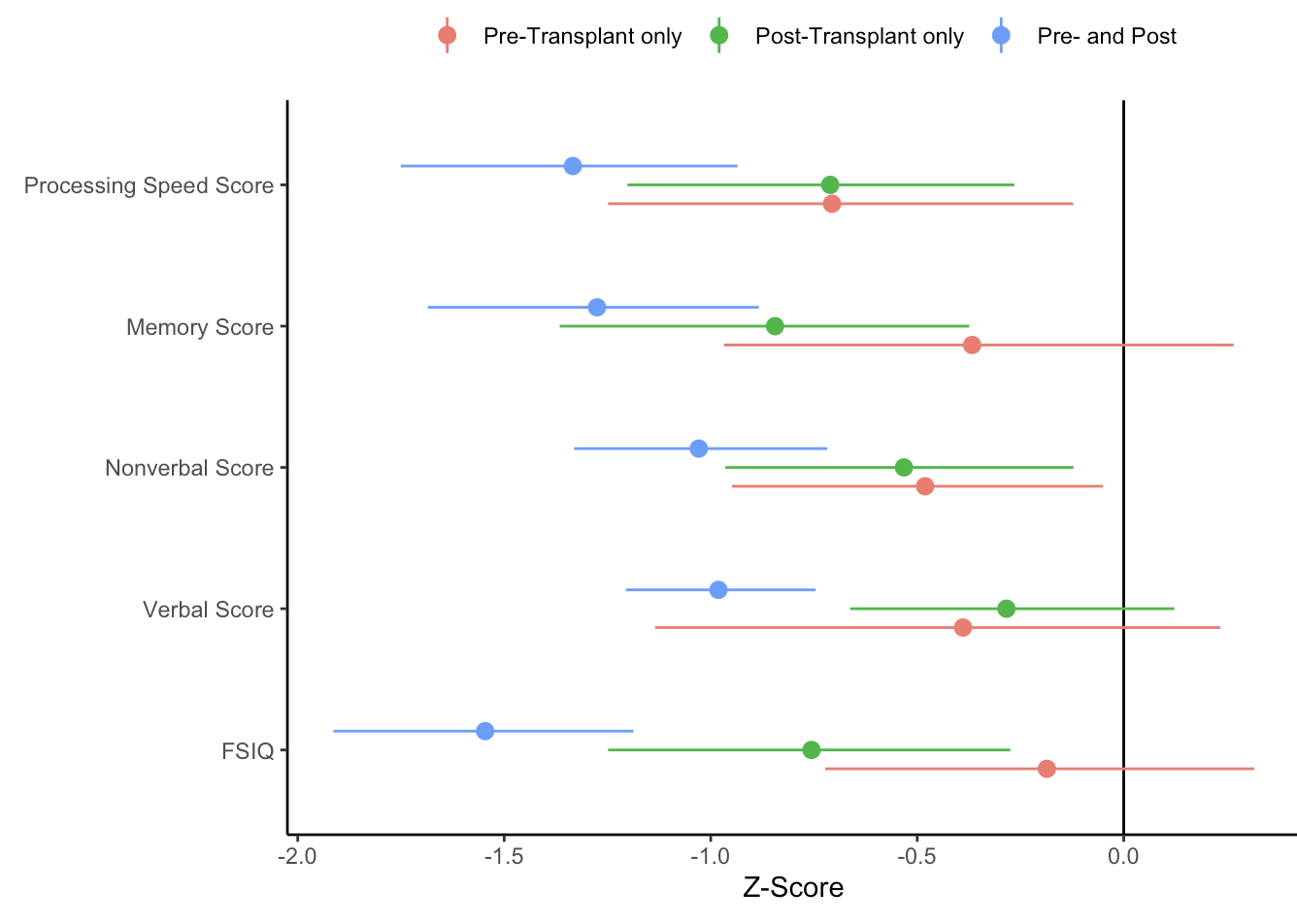 Z-scores were plotted across cognitive measures (y-axis) for each group. Means and 95% confidence limits (CI) are shown. The vertical line at Z=0 marks normal performance.
Z-scores were plotted across cognitive measures (y-axis) for each group. Means and 95% confidence limits (CI) are shown. The vertical line at Z=0 marks normal performance.