Gregory C. Valentine, University of Washington, Tacoma, WA, United States; Kim Boggess, UNC Chapel Hill, Chapel Hill, NC, United States; Kamaira Philips, University of North Carolina at Chapel Hill School of Medicine, Chapel Hill, NC, United States; Carl L. Bose, University of North Carolina at Chapel Hill School of Medicine, Pittsboro, NC, United States; Kevin L. Moss, Unc school of dentistry, Chapel hill, NC, United States; Julie Marchesan, University of North Carolina at Chapel Hill, Chapel Hill, NC, United States; Michael O’Shea, University of North Carolina at Chapel Hill School of Medicine, Chapel Hill, NC, United States; Myriam Peralta-Carcelen, University of Alabama at Birmingham, Birmingham, AL, United States; James D. Beck, University of North Carolina, Chapel Hill, NC, United States
Assistant Professor of Pediatrics, Division of Neonatology University of Washington Tacoma, Washington, United States
Background: Maternal periodontitis causes localized and systemic inflammation. Fetal exposure to maternal infection and inflammation has been associated with development of autism spectrum disorder (ASD). Treatment for periodontitis consists of non-surgical therapy to reduce dental plaque and diminish this infectious and inflammatory burden.
Objective: We sought to determine whether non-surgical periodontal therapy performed in the mid-trimester of pregnancy (intervention) compared to after pregnancy (control) is associated with reduced risk of ASD, as indicated by a screening test, the Modified Checklist for Autism in Toddlers (MCHAT).
Design/Methods: We performed a prospective, follow-up study of the offspring of women enrolled in the Maternal Oral Therapy to Reduce Obstetric Risk (MOTOR) randomized controlled trial. We determined risk of ASD by administering the M-CHAT in toddlers at 2 years of age (+ 2 months). M-CHAT failure was defined as ≥ 2 critical items or ≥3 total items failed. We measured interleukin-6 (IL-6) in cord blood. Mothers had additional IL-6 assessments at enrollment and 48-72 hours after delivery. All examiners were blinded to treatment assignment. Treatment effect was described as the risk of a failed M-CHAT among those in the intervention group relative to the risk among controls.
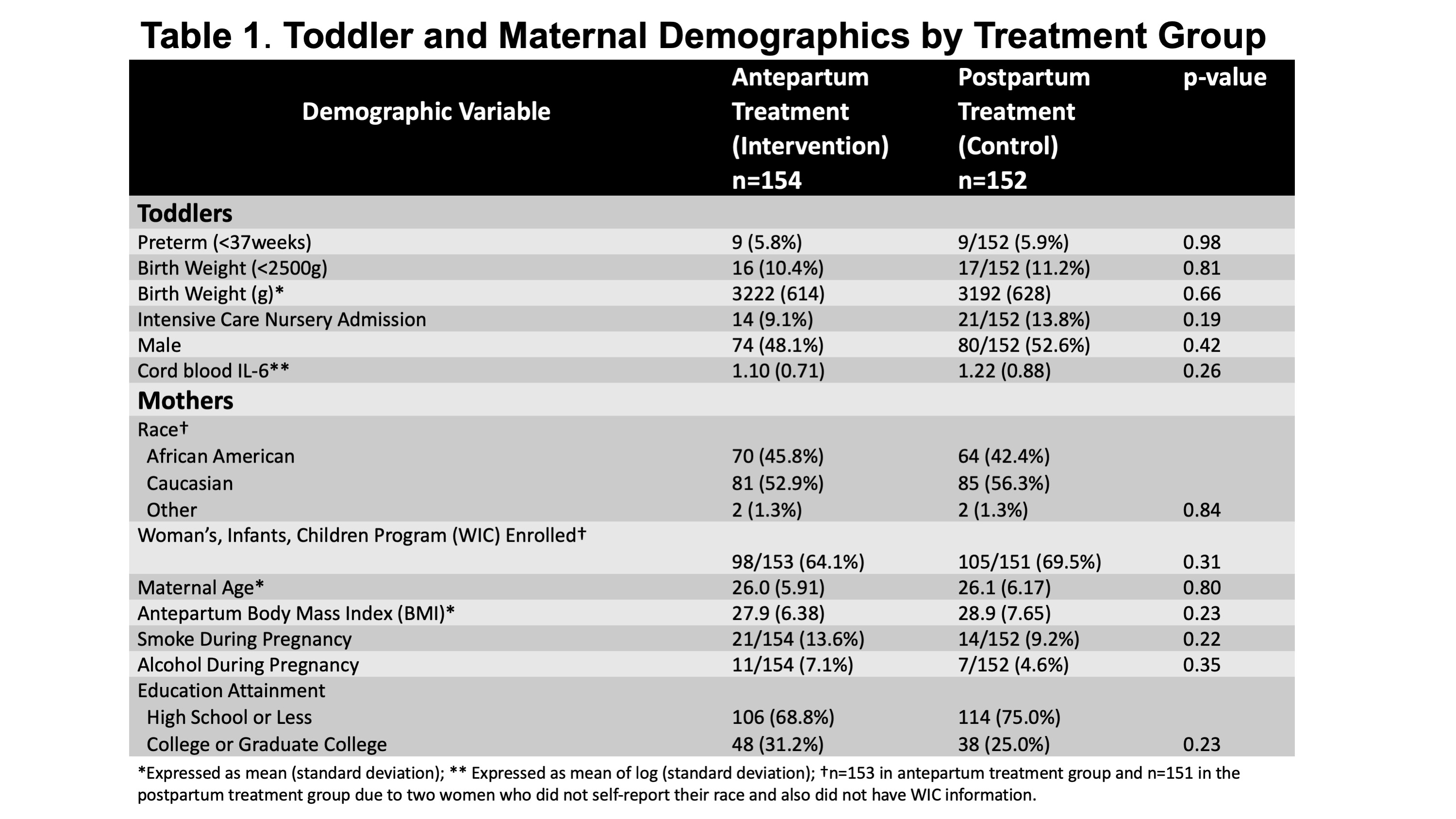
Results: We evaluated 306 2-year-olds. There were no baseline maternal or neonatal demographic differences based on treatment group (Table 1), but more toddlers who failed the M-CHAT than those who passed were born to self-described Caucasian mothers (78% vs 51%, p=0.008). Toddlers of women in the intervention group had a significantly decreased risk of M-CHAT failure (adjusted RR=0.53, 95% CI 0.29-0.99; Table 2). Mean IL-6 in cord blood and maternal IL-6 change from baseline was higher among offspring who failed the M-CHAT compared to those who passed (new Table 3; p=0.001 and 0.03, respectively).Conclusion(s): Treating periodontal disease during pregnancy was associated with a reduced risk of ASD, as measured by the M-CHAT. Reduction in an inflammatory marker (IL-6) is associated with lower risk of failing the M-CHAT. Considering that autism etiology implicates genetic and intrauterine exposures, antepartum periodontal treatment to reduce fetal exposure to maternal infection and inflammation may help prevent development of ASD. Table 1: Toddler and Maternal Demographics by Treatment Group Table 2: M-CHAT Outcomes by Treatment Group