Neonatal Respiratory II: Respiratory Physiology and Devices
457 - Work of breathing indices and oxygen saturation at discharge in premature infants with history of respiratory insufficiency
Saturday, April 23, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 457 Publication Number: 457.228
Kelley Z. Kovatis, Christiana Care, Philadelphia, PA, United States; Robert Locke, Christiana Care/Sidney Kimmel School of Medicine at Jefferson Univ, Newark, DE, United States; Amy Mackley, Christiana Care Health System, Newark, DE, United States; Thomas H. Shaffer, NemoursAlfred I. duPont Hospital for Children, Wilmington, DE, United States
Attending Physician Christiana Care Newark, Delaware, United States
Background: Premature infants commonly demonstrate Thoracoabdominal asynchrony (TAA) secondary to highly compliant rib cage and poor compensation by immature respiratory muscles. Increased TAA signifies increased work of breathing (WOB). Respiratory inductive plethysmography (RIP) is a noninvasive way to objectively assess TAA and quantify WOB. Normative WOB data for premature infants at discharge has not been established.
Objective: To establish normal WOB indices [phase angle(Փ), labor breathing index (LBI), HR, Saturations) at discharge for premature infants in the supine position (S) and in the car seat test (CST).
Design/Methods: This is a prospective observational study of infants born with a birth weight of < 1500 grams and at >26-week gestation at a single center NICU. Infants had RIP and pulse oximetry measurements (mean +/- SEM) in the S position and during the CST within 7 days of discharge. PneuRIP, a portable, bedside software provided real time clinical data. Diagnosis of BPD was based on the 2018 NICHD criteria. Փ>40 and LBI> 1.15 suggests respiratory distress in pediatric populations.
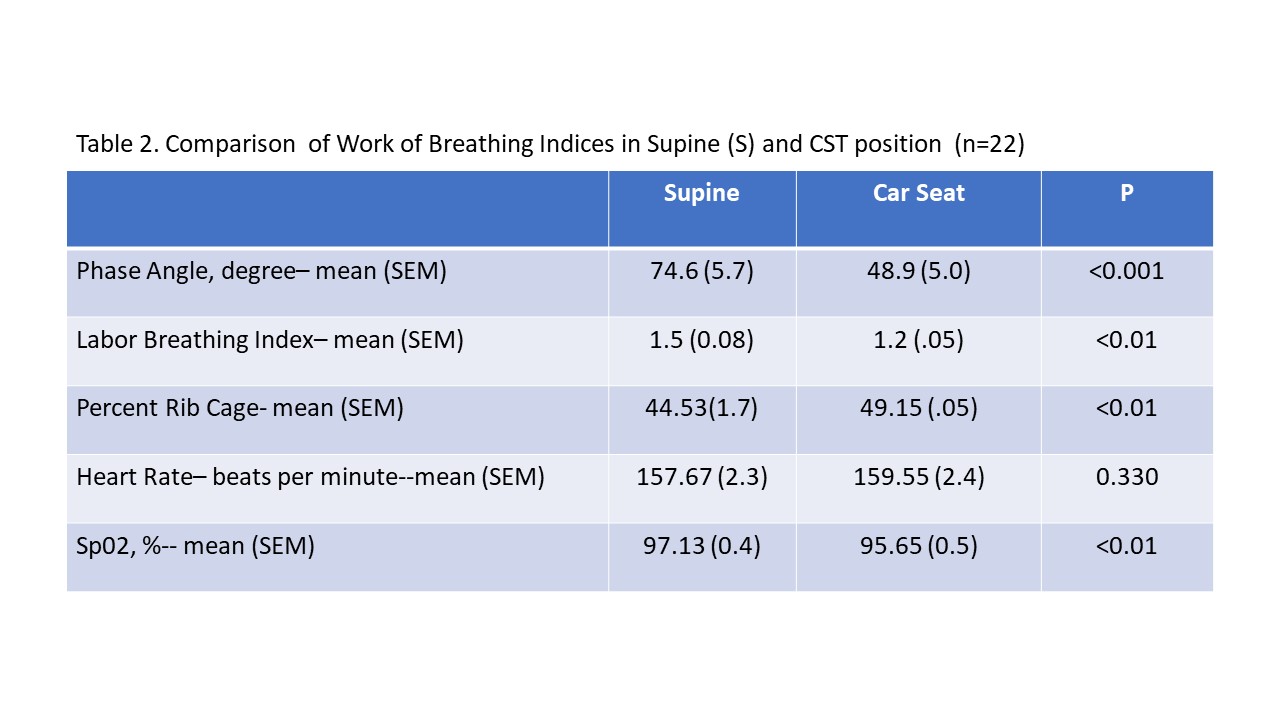
Results: Preliminary data includes 30 of the anticipated 62 infants. The Փ in the S position is 720±5, (Table 1). There is no difference in WOB indices in the S position for infants with BPD vs Control. Infants with BPD had lower HR [150±4 vs 161±2; p < 0.01] and saturations [95%±1 vs 99%±0.3; p < 0.01]. We observed Increased WOB indices in the S position compared to the CST [Փ: 750±6 vs 490±5; p < 0.001]. Infants in the CST had statistically but not clinically lower saturations [96%±1 vs 97%±0.4; p < 0.01] (Table 2). Infants with Փ >900 (70th percentile), demonstrated significantly improved WOB indices during the CST [Փ:1080±2 vs 570±15, p=.02) (Fig 1). Infants with BPD have increased WOB indices in the CST compared to controls [Փ: 680±14 vs 420±3.3; p < 0.01] and LBI: [1.4±0.2 vs 1.2±0.1; p < 0.05].Conclusion(s): Premature infants at discharge have increased WOB indices relative to the older pediatric population. Position (S vs CST) at discharge affects WOB indices. BPD and/or increased WOB indices at discharge may impact guidelines for patient position , discharge criteria and respiratory support. Table 1. Summary of Work of Breathing Indices in the Supine (S) Position Table 2. Comparison of Work of Breathing Indices in Supine (S) and CST position


.jpg)