397 - Electronic Triggers to Study Diagnostic Errors in Pediatric Emergency Departments
Sunday, April 24, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 397 Publication Number: 397.315
Prashant Mahajan, University of Michigan Medical School, Ann Arbor, MI, United States; Emily N. White, University of Michigan - Department of Biostatistics, Ann Arbor, MI, United States; Elizabeth R. Alpern, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; James Chamberlain, Children's National Health System, Washington, DC, United States; Richard M. Ruddy, University of Cincinnati College of Medicine, Cincinnati, OH, United States; Kathy N. Shaw, University of Pennsylvania Perelman School of Medicine, Philadelphia, PA, United States; Michele Carney, University of Michigan Medical School, Ann Arbor, MI, United States; Jacqueline B. Corboy, Ann & Robert H. Lurie Children's Hospital of Chica, Wilmette, IL, United States; Andrew T. Krack, Children's Hospital Colorado, Highlands Ranch, CO, United States; Brandon Ku, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Daphne Morrison Ponce, Uniformed Services University of the Health Sciences F. Edward Hebert School of Medicine, Portsmouth, VA, United States; Nicole Klekowski, University of Michigan Medical School, Ann Arbor, MI, United States; Karen O'Connell, The George Washington University School of Medicine and health sciencez, Upper Marlboro, MD, United States; Asha S. Payne, Children's National Health System, Washington, DC, United States; Elizabeth A. Freiheit, University of Michigan, ANN ARBOR, MI, United States; Hardeep Singh, Baylor College of Medicine, Houston, TX, United States
Professor of Pediatrics and Emergency Medicine University of Michigan Medical School Ann Arbor, Michigan, United States
Background: Diagnostic errors, framed as missed opportunities for improving diagnosis (MOIDs), lead to safety concerns in pediatric emergency departments (EDs). We sought to identify triggers to screen ED records for diagnostic errors.
Objective: After pilot testing, we applied three electronic triggers (eT) to study frequency and contributory factors of diagnostic errors in pediatric EDs: return visits within 10 days resulting in admission (eT1), care escalation to intensive care unit within 24 hours of ED presentation (eT2), and death within 24 hours of ED visit (eT3).
Design/Methods: We created a standardized electronic query and reporting template for the 3 eTs and applied them to electronic health record systems of 5 pediatric EDs. Using ED visits from 2019, we included a random subset of 400 ED visits for eT1 and all visits for eT2 and eT3 at each site. We trained 2 clinicians from each ED to review the triggered cases. Each reviewer manually screened the chart and initially categorized charts as “unlikely for MOIDs” or “unable to rule out MOIDs” without a detailed chart review. For the latter category, reviewers performed a detailed chart review using the Revised Safer Dx Instrument to categorize as MOIDs or no MOIDs, dichotomized as a score ≥ 5 out of 7 on a Likert scale as suggestive of a MOID.
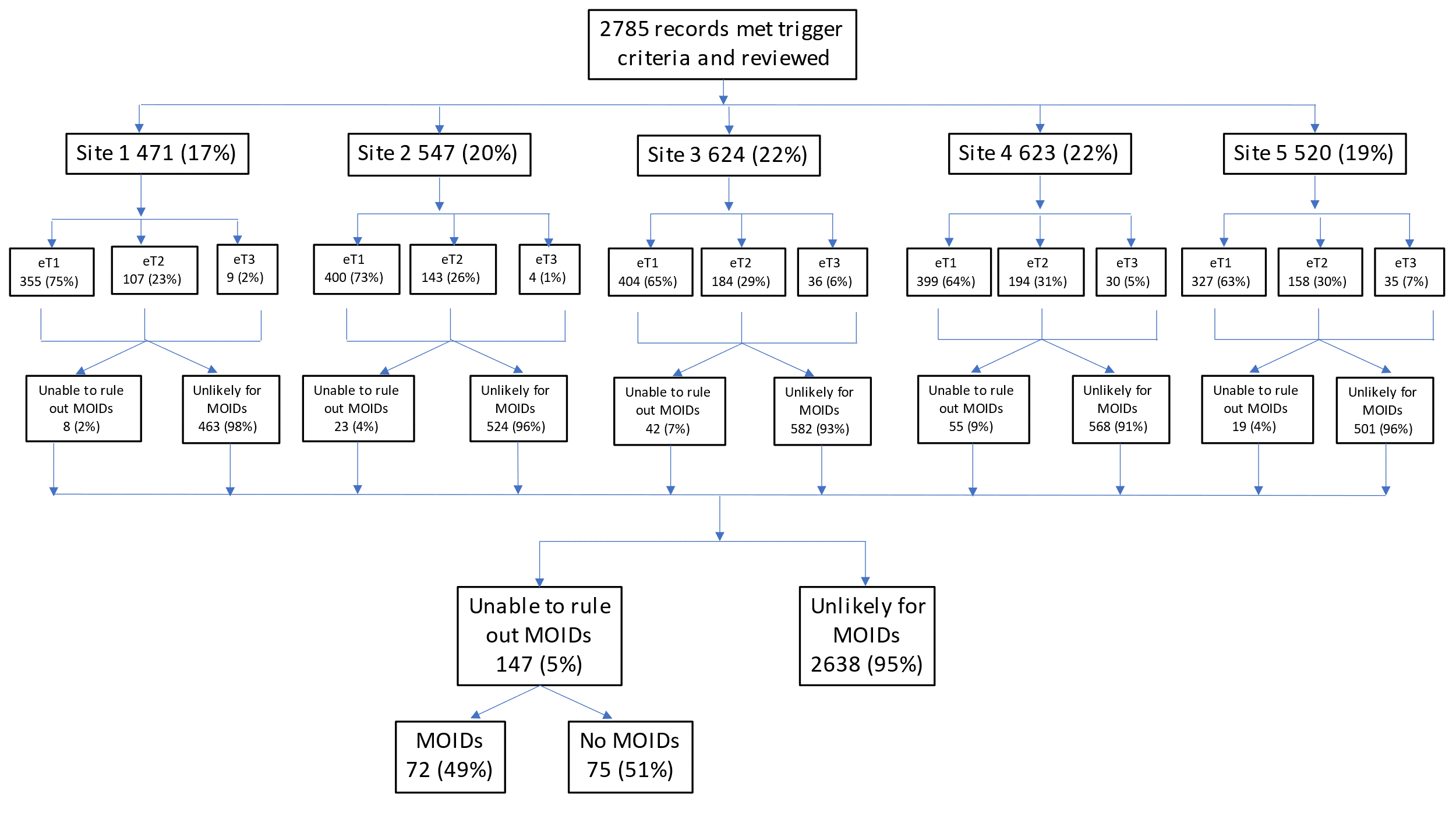
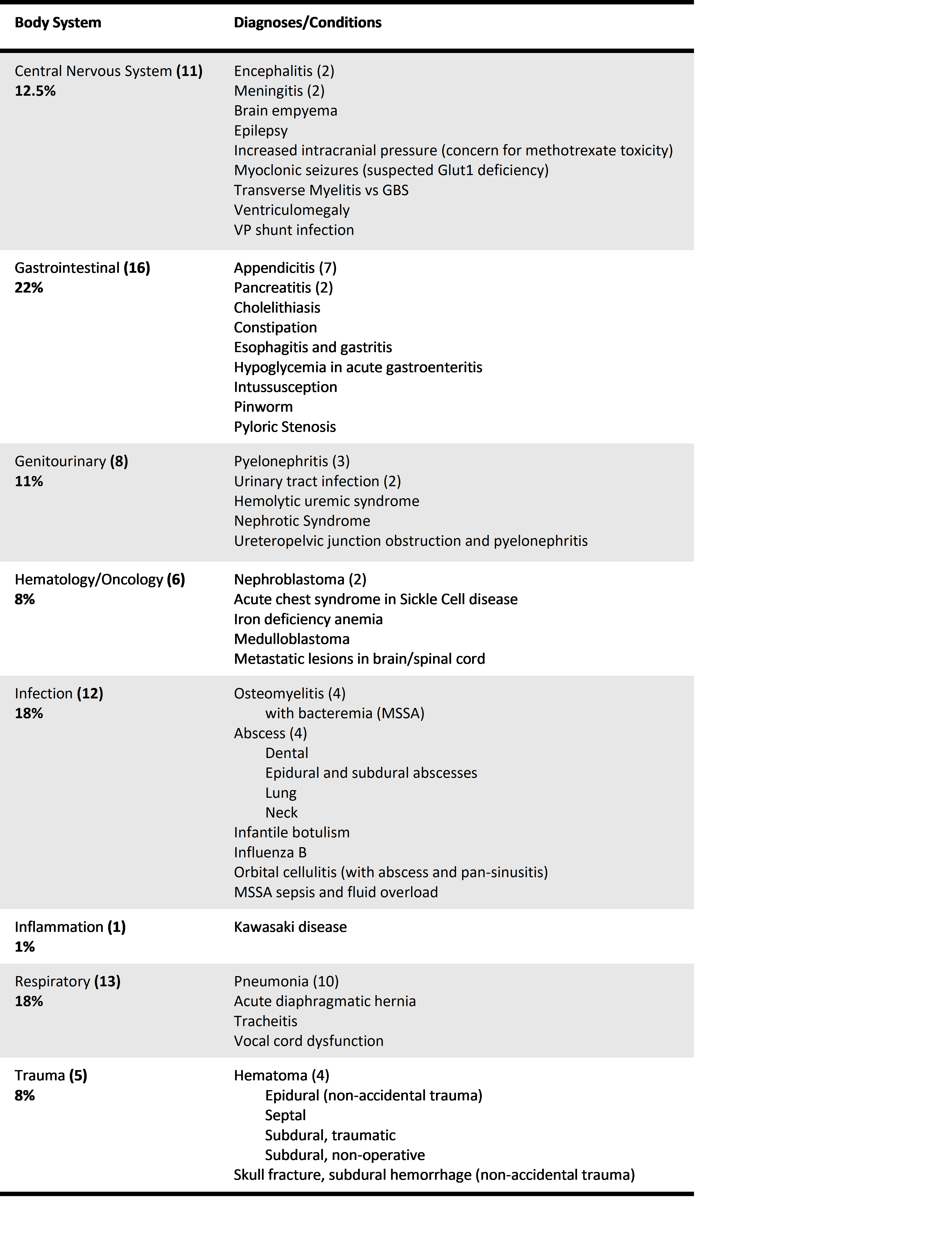
Results: 2785 ED records met trigger criteria (eT1 1885 (68%), eT2 786 (28%), and eT3 114 (4%)), of which 2638 (95%) were categorized as unlikely for MOIDs (Figure 1). The Safer Dx Instrument was applied to 147 (5%) records and 72 (49%) had MOIDs. The proportion of charts with MOIDs ranged from 0.6% to 4.3% across sites. The overall frequency of MOIDs in the triggered charts was 2.6% (72/2785) for the entire cohort, 3.0% (57/1885) for e-trigger1, 1.9% (15/786) for e-trigger2, and 0% (0/114) for e-trigger3. The most common diagnoses associated with MOIDs were pneumonia (10/72) and appendicitis (7/72) (Table 1). 54% (39/72) had patient harm due to MOIDs. Contributing factors, although difficult to determine retrospectively, were most often assigned to patient-provider factors (36/72), followed by patient factors (16/72), system factors (10/72), and provider factors (8/72) (Table 2).Conclusion(s): Electronic triggers with selective record review is an efficient way to screen large numbers of medical records to identify diagnostic errors in pediatric ED visits. Detailed chart review of 5% of charts revealed MOIDs in half, of which half were harmful. Triggers can be an integral part of diagnostic safety measurement systems and identify cases for additional review, analysis, and improvement. Consort Diagram Categorizing 72 missed opportunities for improving diagnosis by body system (by frequency, then alphabetical)